The creation and management of psychiatric progress notes are a cornerstone of effective patient care within the mental health field. These detailed records provide a comprehensive overview of a patient’s progress, challenges, and treatment plan, facilitating collaboration among providers, caregivers, and the patient themselves. A well-structured psychiatric progress note template is not merely a document; it’s a vital tool for continuity of care and informed decision-making. Psychiatric Progress Note Template is a standardized format designed to capture essential information, ensuring consistent documentation and facilitating accurate analysis. This article will delve into the key components of a robust psychiatric progress note, exploring its importance, best practices, and variations to suit different clinical settings. Understanding how to effectively utilize this template can significantly improve patient outcomes and streamline workflows.
The Importance of Psychiatric Progress Notes
The initial implementation of psychiatric progress notes was driven by a desire to improve patient safety and accountability. Before standardized templates, clinicians often relied on fragmented notes, leading to inconsistencies in documentation and potential for errors. Today, these templates are essential for several reasons:
- Improved Patient Safety: Consistent documentation reduces the risk of miscommunication and ensures that crucial information is readily available to all involved.
- Enhanced Continuity of Care: A standardized format facilitates seamless transitions between providers, ensuring patients receive consistent and coordinated care.
- Data Collection & Analysis: Progress notes provide a valuable source of data for tracking treatment effectiveness, identifying trends, and evaluating the impact of interventions.
- Legal and Regulatory Compliance: Many insurance companies and regulatory bodies require detailed documentation of patient care.
- Patient Empowerment: Having a readily available record of their treatment history empowers patients to actively participate in their care.
Core Components of a Psychiatric Progress Note
A comprehensive psychiatric progress note typically includes several key sections. Each section is designed to address a specific aspect of the patient’s care. Let’s examine these components in detail:
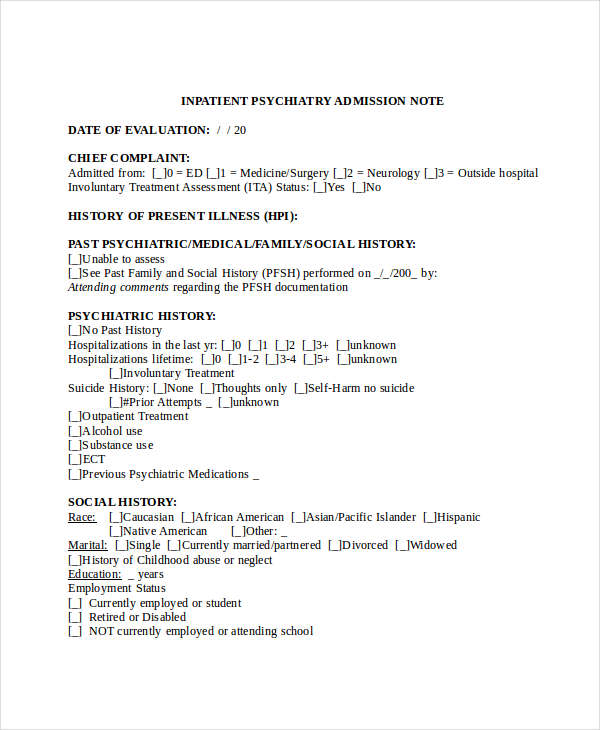
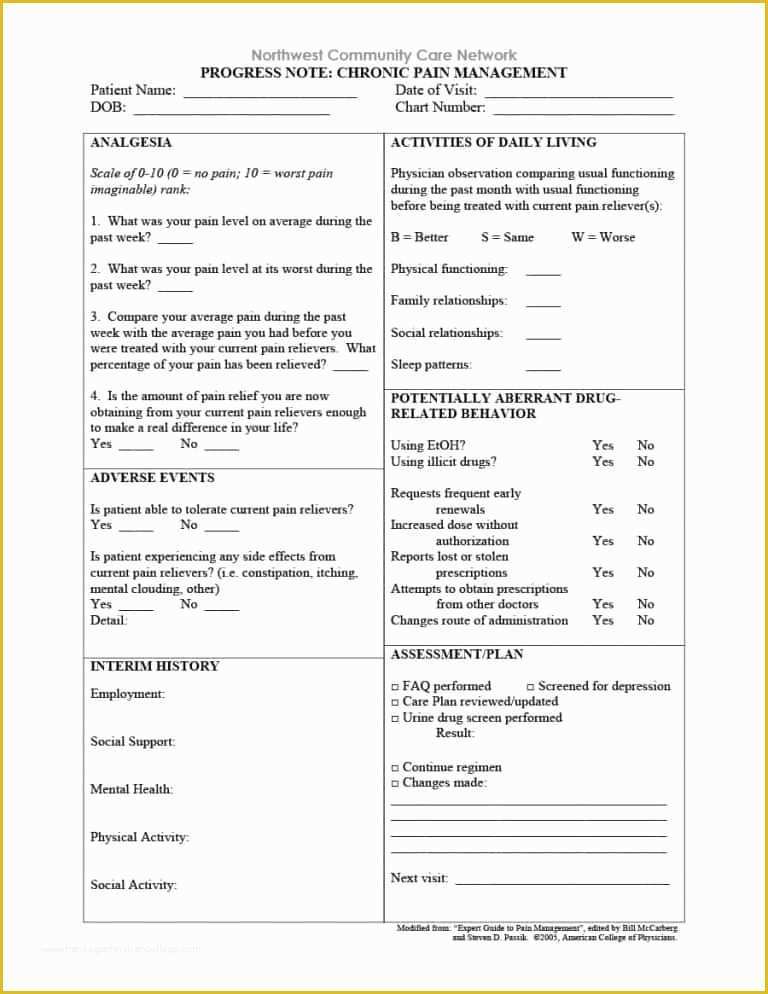
1. Patient Demographics & Initial Assessment
This initial section gathers essential information about the patient, including:
- Patient Name: Full name and date of birth.
- Date of Birth: Crucial for accurate record-keeping.
- Contact Information: Phone number and email address.
- Insurance Information: Necessary for billing and insurance purposes.
- Initial Assessment: A brief summary of the patient’s presenting problem, including the primary symptoms and concerns. This section often includes a brief clinical interview.
- Relevant Medical History: Including any significant past medical conditions, allergies, and current medications.
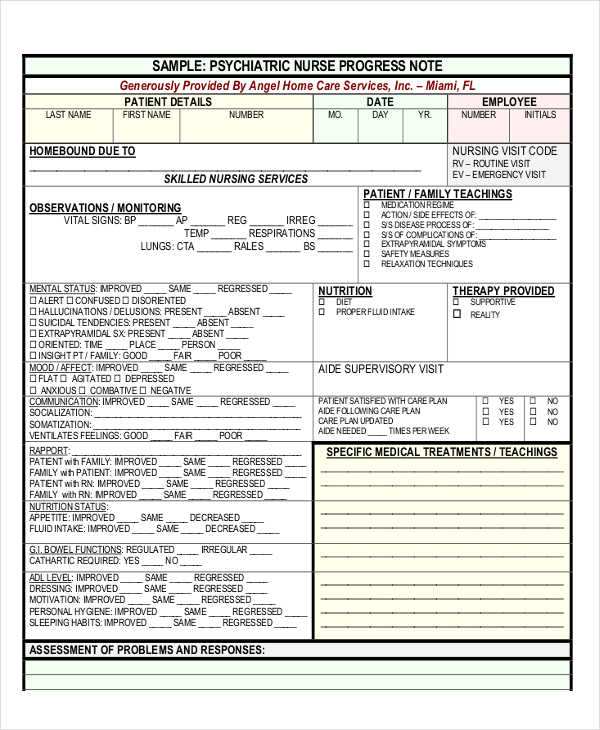
2. Current Status & Symptoms
This section provides a detailed description of the patient’s current mental state, including:
- Mood: Patient’s current emotional state (e.g., depressed, anxious, irritable).
- Cognition: Level of alertness, concentration, and memory.
- Behavior: Observations of behavior, including any changes in eating, sleeping, or social interaction.
- Thought Patterns: Description of any unusual or distressing thoughts.
- Sleep Patterns: Details about sleep quality and duration.
- Substance Use: Assessment of any substance use history and current substance use.
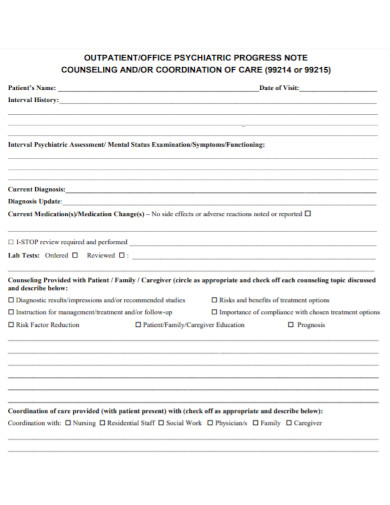
3. Treatment Plan & Interventions
This section outlines the treatment plan currently in place, including:
- Medication Review: Current medications, dosages, and any changes made.
- Therapy Sessions: Details of therapy sessions, including the therapist’s approach and the patient’s response.
- Psychosocial Interventions: Description of any psychosocial interventions being used (e.g., cognitive behavioral therapy, social skills training).
- Lifestyle Modifications: Recommendations for lifestyle changes (e.g., diet, exercise, sleep hygiene).
4. Progress & Response to Treatment
This is arguably the most critical section, detailing the patient’s response to treatment. It includes:

- Treatment Effectiveness: Assessment of whether the treatment is achieving the desired outcomes. This might be quantified with specific metrics (e.g., reduction in symptoms, improvement in mood).
- Challenges Encountered: Description of any difficulties the patient is experiencing, and how these challenges are being addressed.
- Patient Feedback: Direct feedback from the patient regarding their experience with treatment.
- Potential Side Effects: Any adverse effects of medications or therapies.
5. Further Assessment & Planning
This section identifies any further assessments needed, and proposes future treatment goals.
- Diagnostic Testing: Any planned or completed diagnostic testing (e.g., blood tests, brain imaging).
- Referrals: Any referrals to other specialists (e.g., psychiatrist, neurologist).
- Goals & Objectives: Specific, measurable, achievable, relevant, and time-bound (SMART) goals for future treatment.
Variations and Considerations for Psychiatric Progress Note Templates
While the core components remain consistent, different psychiatric progress note templates may be used depending on the setting and the specific needs of the patient.

- Acute Care: In acute care settings, the note will be more detailed and focused on immediate needs.
- Long-Term Care: For long-term care patients, the note may include more detailed information about functional limitations and support services.
- Telehealth: Telehealth progress notes require specific formatting and data capture protocols.
- Electronic Health Records (EHRs): Many EHR systems offer templates and tools to streamline progress note creation.
The use of standardized templates is not a one-size-fits-all solution. However, a well-designed template provides a framework for consistent and comprehensive documentation, ultimately contributing to improved patient care.

Conclusion
Psychiatric progress notes are an indispensable tool in the mental health profession. They represent a critical component of patient care, facilitating continuity of care, data collection, and informed decision-making. By understanding the core components of a robust psychiatric progress note template and adapting it to specific clinical needs, clinicians can significantly enhance the quality of patient care and contribute to positive outcomes. The consistent application of this template, coupled with a commitment to thorough documentation, is paramount for ensuring effective treatment and promoting patient well-being. Psychiatric Progress Note Template is a vital instrument for achieving these goals.
Conclusion
The creation and management of psychiatric progress notes are a cornerstone of effective patient care within the mental health field. Standardized templates are essential for improving patient safety, enhancing continuity of care, and facilitating data collection. A well-structured progress note provides a comprehensive record of a patient’s progress, enabling clinicians to make informed decisions and ultimately improve outcomes. The consistent use of a standardized template, coupled with a commitment to thorough documentation, is paramount for achieving these goals. Psychiatric Progress Note Template is a vital instrument for achieving these goals.