The demand for efficient and accurate patient care is constantly increasing, placing a significant burden on healthcare professionals. Nurses play a pivotal role in this process, meticulously documenting patient information and providing vital care. A well-structured nurse report template is an indispensable tool for ensuring continuity of care, facilitating communication between healthcare providers, and supporting informed decision-making. This guide will delve into the essential components of a robust nurse report template, exploring its purpose, structure, and best practices. Nurse Report Template is more than just a document; it’s a critical communication tool that safeguards patient safety and enhances overall clinical efficiency. Understanding its nuances is crucial for nurses seeking to optimize their workflow and deliver the best possible care. This article will provide a detailed overview of what to include and how to format a truly effective nurse report template.
Understanding the Purpose of a Nurse Report Template
The primary purpose of a nurse report template is to systematically record patient information, observations, and interventions. It’s a standardized format designed to capture crucial details quickly and accurately, allowing healthcare providers to readily access the necessary information when needed. Without a consistent template, nurses risk losing valuable data, leading to potential errors and compromised patient care. Furthermore, a well-structured report facilitates collaboration among team members, ensuring everyone is on the same page regarding patient status and treatment plans. It’s a vital component of quality patient care and demonstrates a commitment to thorough documentation. The template streamlines the reporting process, saving time and reducing the potential for errors associated with manual note-taking. It’s a cornerstone of effective patient management.
Core Sections of a Nurse Report Template
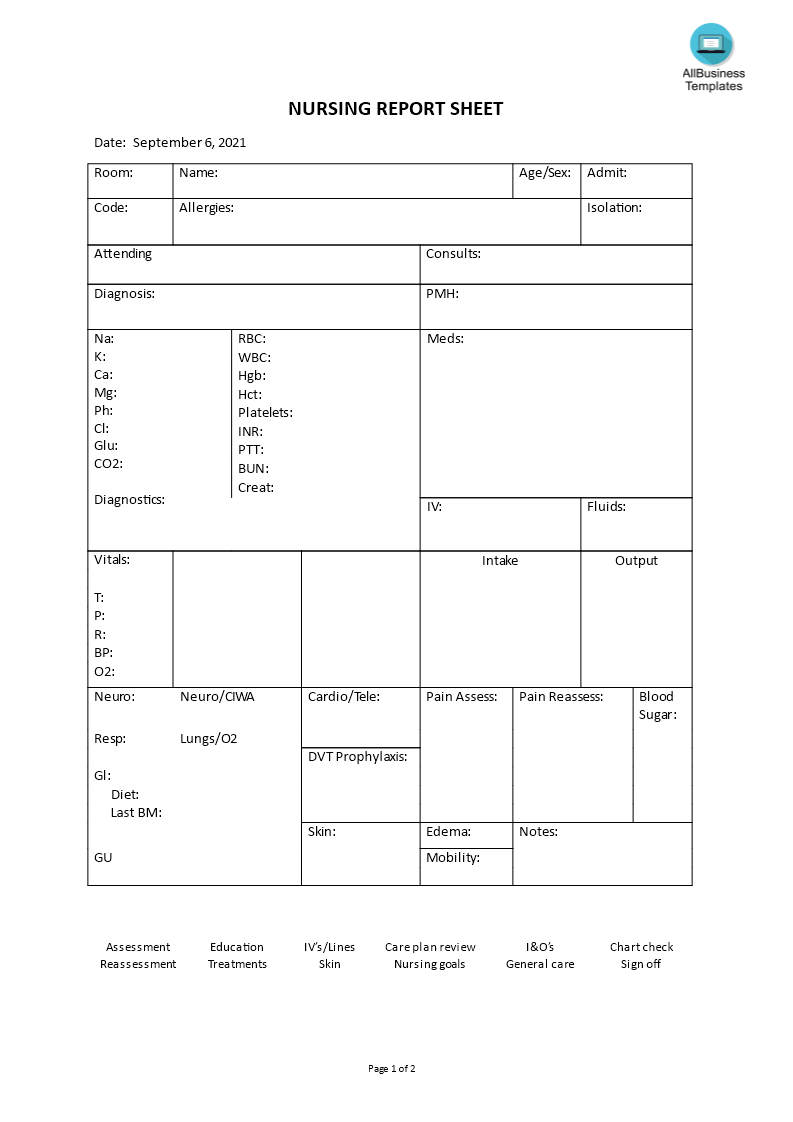
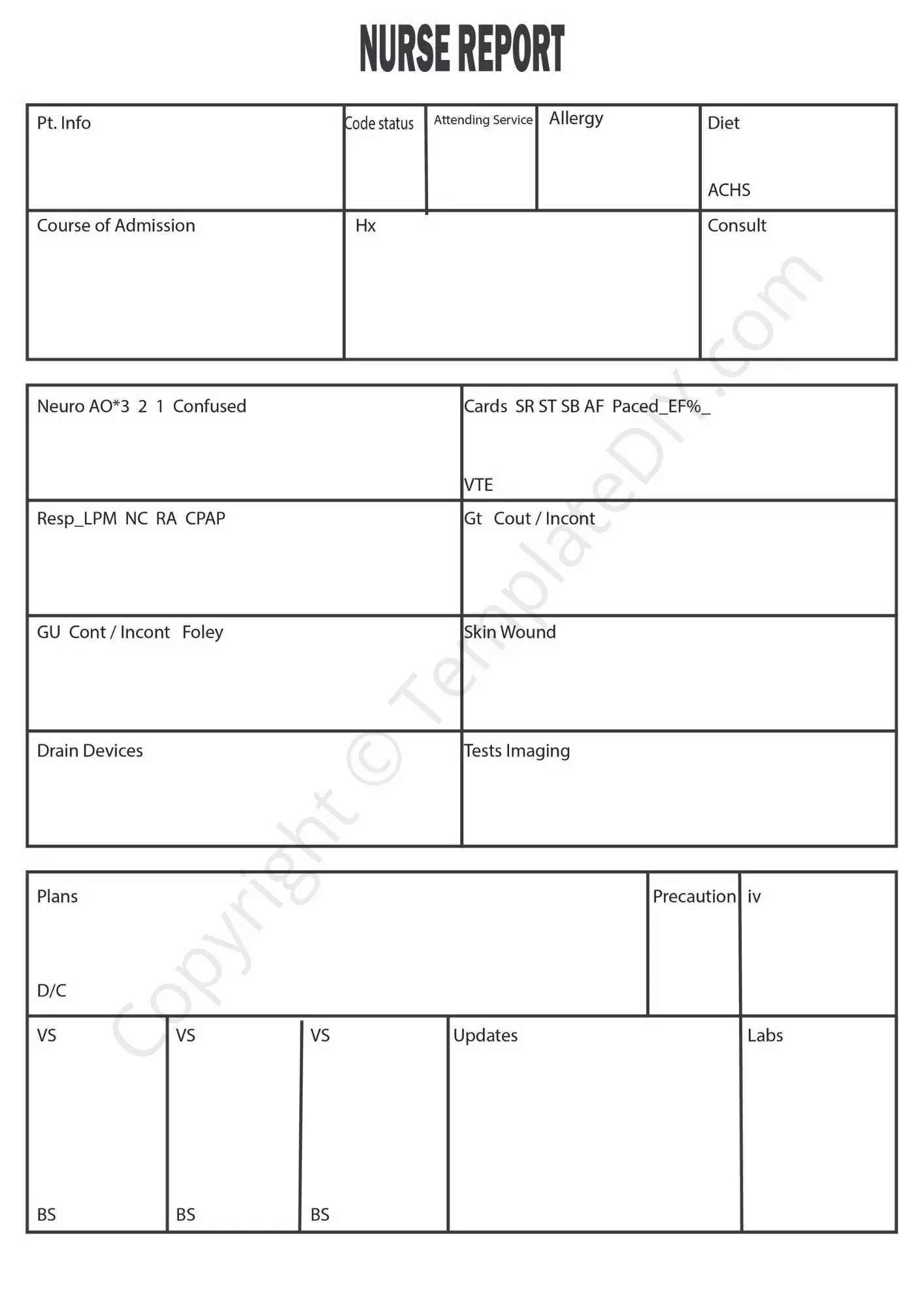
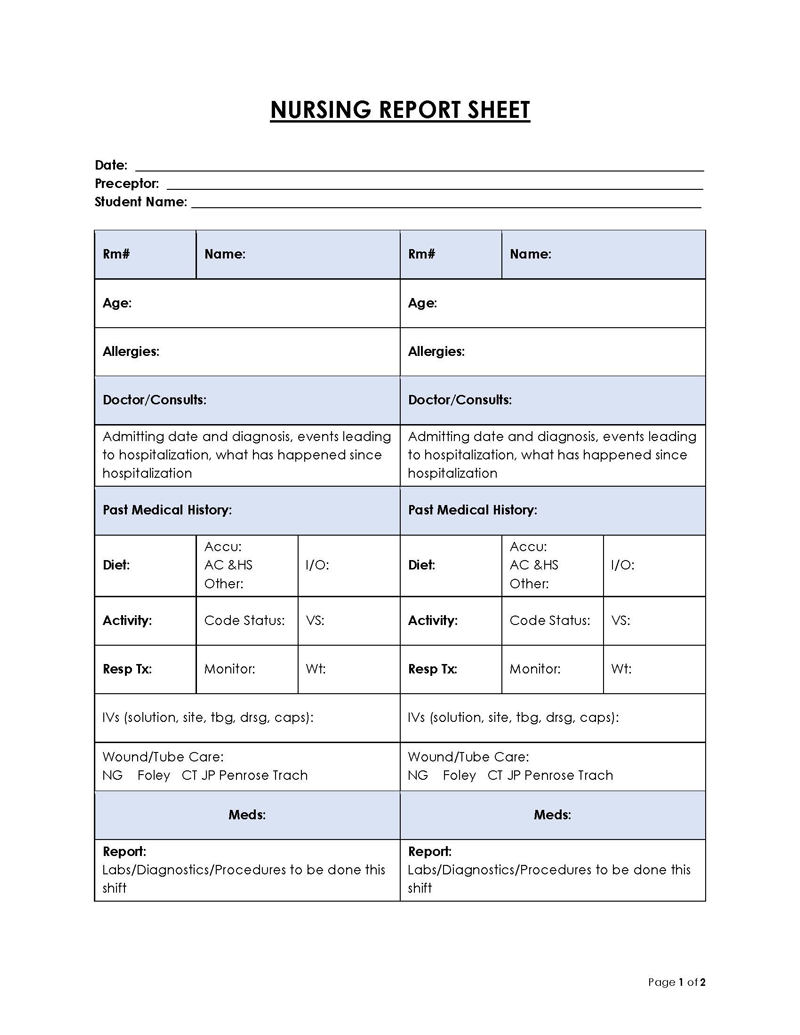
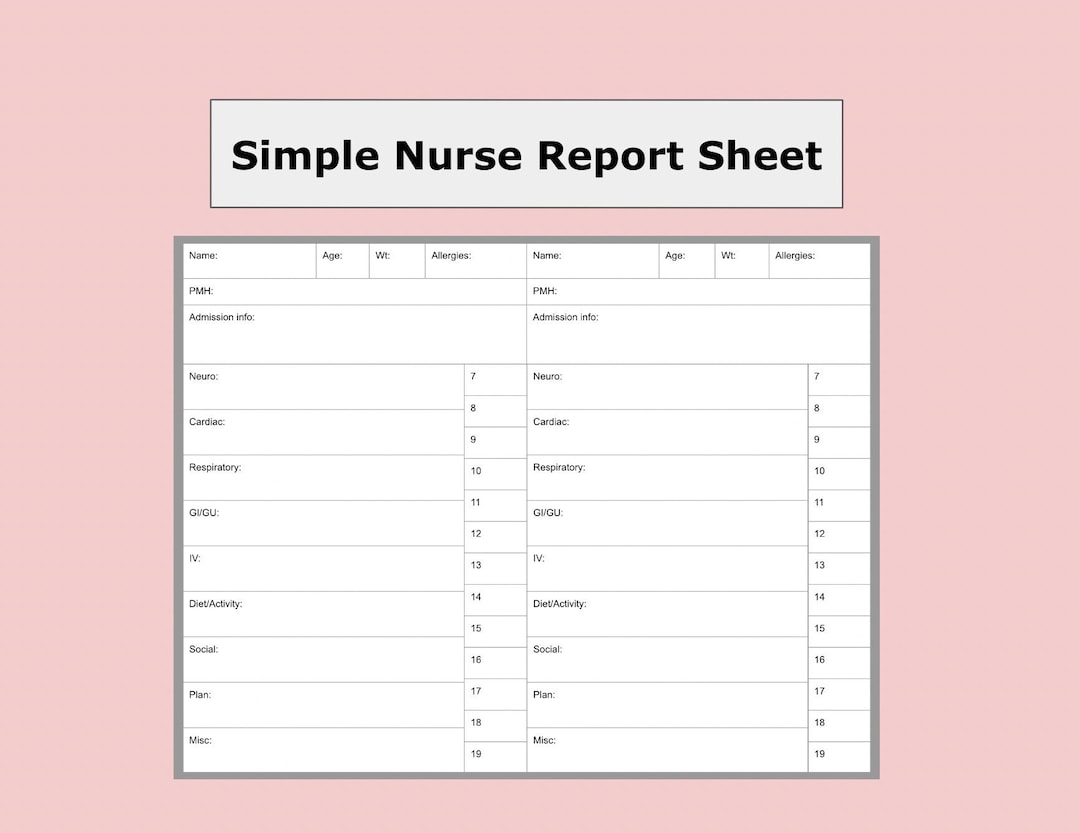
A comprehensive nurse report template typically includes the following key sections:

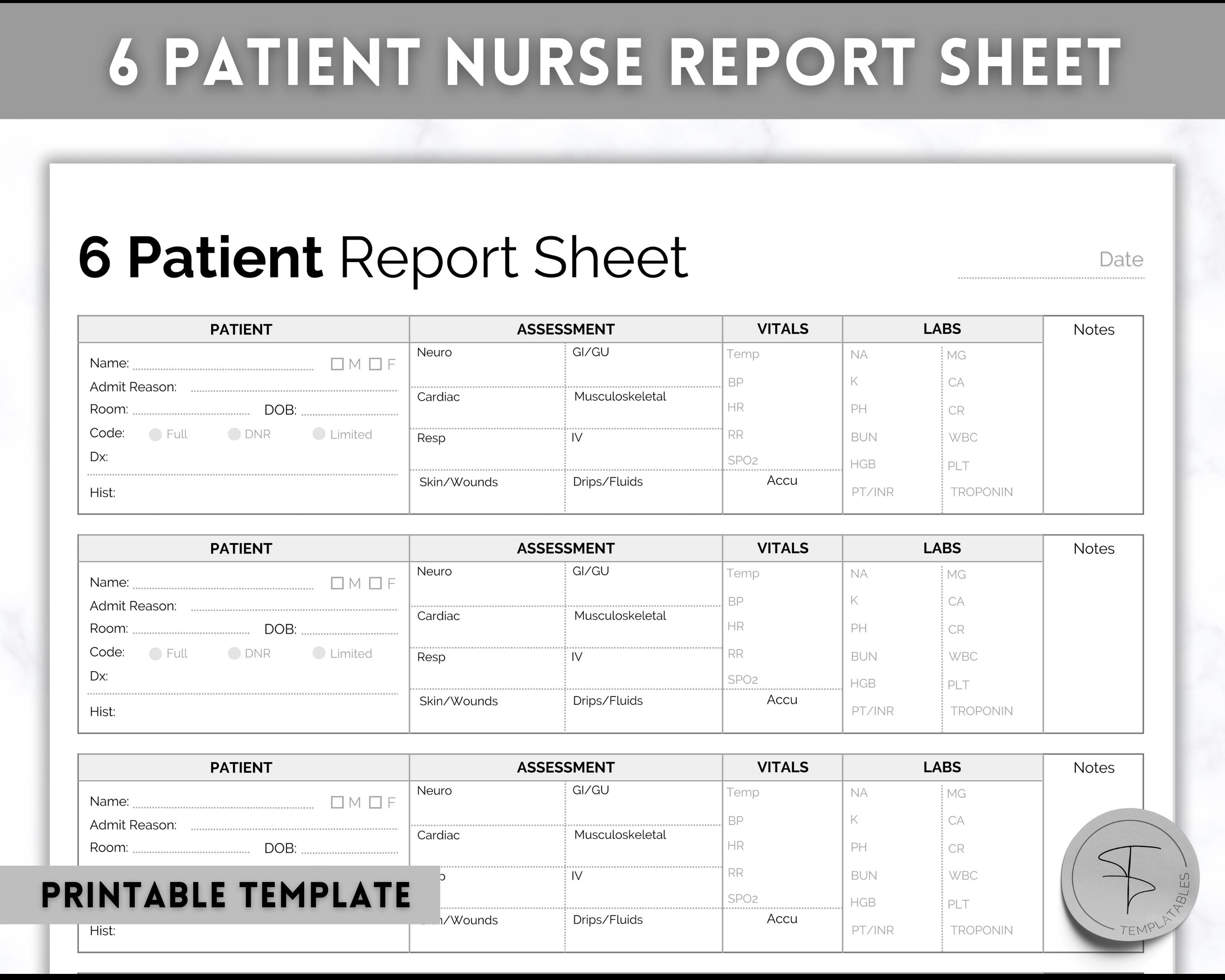
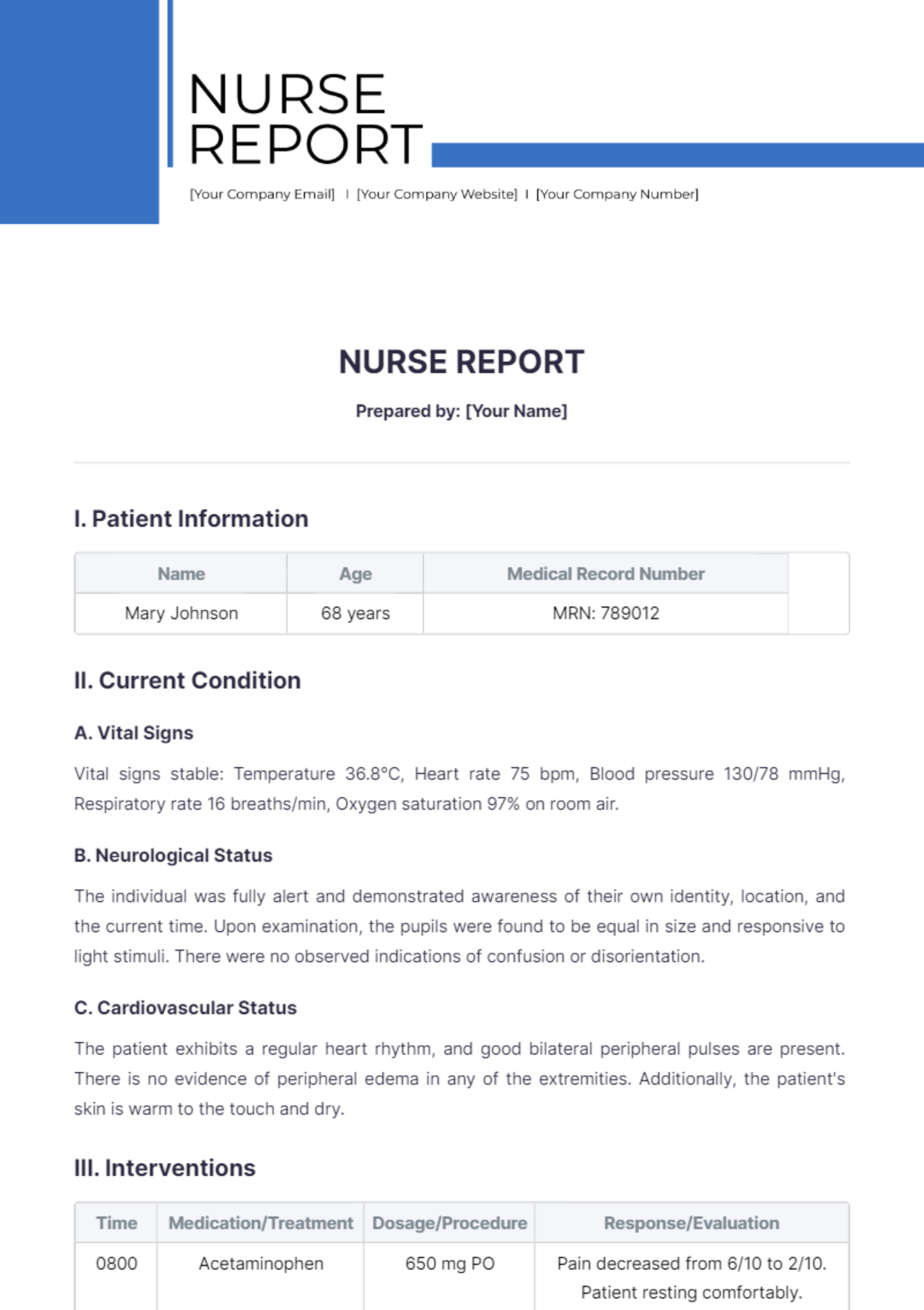
1. Patient Demographics
This section provides essential information about the patient, ensuring easy identification and tracking. It includes:

- Patient Name: Full name, including any nicknames or preferred titles.
- Date of Birth: Crucial for accurate identification and tracking of patient history.
- Medical Record Number (MRN): Unique identifier for each patient.
- Contact Information: Phone number, address, and emergency contact details.
- Insurance Information: Policy number and group name.
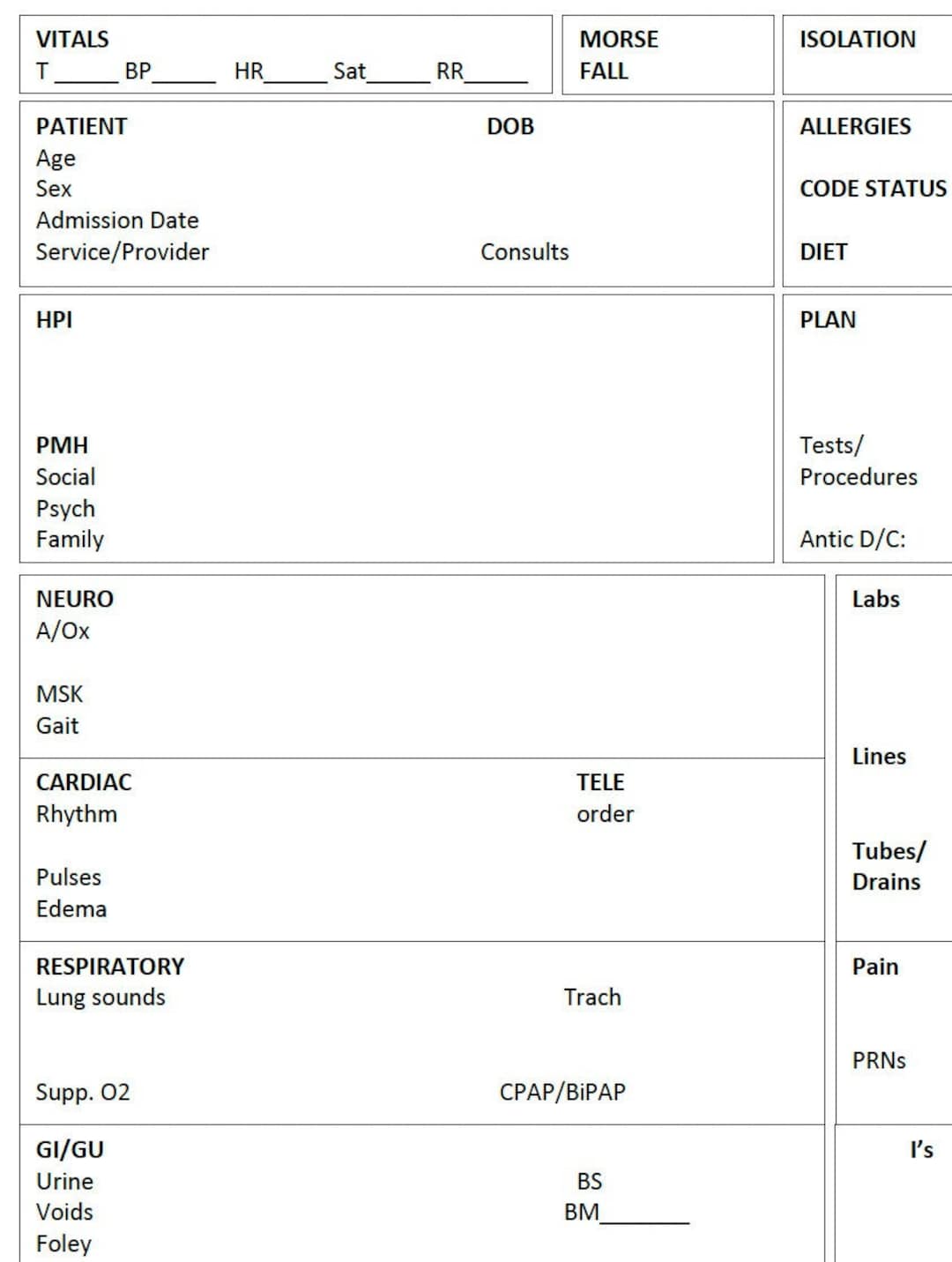
2. Assessment Findings
This section details the patient’s current condition, based on observations and assessments. It’s a critical area for documenting vital signs, physical examination findings, and any relevant diagnostic tests.
- Vital Signs: Temperature, pulse, respiration rate, blood pressure, and oxygen saturation.
- Physical Examination: Observations related to appearance, mobility, and functional status. Note any abnormalities or noteworthy findings.
- Diagnostic Results: Results of laboratory tests, imaging studies, and other diagnostic procedures. Include dates and specific values.
- Differential Diagnosis: A list of potential diagnoses based on the assessment findings.
3. Nursing Interventions
This section outlines the nursing actions taken to address the patient’s needs and concerns. It demonstrates the nurse’s proactive approach to patient care.
- Medication Administration: Details of medications administered, including dosage, route, and time.
- Vital Care Measures: Actions taken to maintain or stabilize the patient’s vital signs.
- Patient Education: Information provided to the patient or their family regarding their condition, treatment plan, and self-care instructions.
- Comfort Measures: Actions taken to alleviate pain, discomfort, or anxiety.
4. Problem List & Plan
This section identifies any problems encountered during the patient’s care and outlines a plan to address them. It’s a crucial element for tracking progress and ensuring continuity of care.
- Problem List: A concise list of any issues that arose during the patient’s care.
- Plan of Care: Specific actions to address each problem, including interventions, follow-up appointments, and referrals.
5. Additional Notes & Observations
This section allows for any additional relevant information that doesn’t fit into the other sections. It’s a space for detailed observations, thoughts, and concerns.
- Patient’s Mood/Emotional State: Note any changes in the patient’s demeanor or emotional response.
- Patient’s Concerns: Address any concerns the patient may have expressed.
- Relevant History: Include any pertinent information from the patient’s chart or previous conversations.
Enhancing the Nurse Report Template: Best Practices
Beyond the core sections, several best practices can significantly improve the effectiveness of a nurse report template:
- Use Clear and Concise Language: Avoid jargon and overly complex sentences. Write in a way that is easily understood by all healthcare providers.
- Be Specific and Detailed: Provide as much relevant information as possible. Avoid vague descriptions.
- Maintain a Consistent Format: Use consistent formatting for headings, bullet points, and dates.
- Utilize Standardized Terminology: Employ established medical terminology to ensure clarity and accuracy.
- Attach Relevant Documents: Include copies of relevant test results, imaging reports, and medication lists.
- Digital Version: Consider utilizing a digital nurse report template for improved accessibility and efficiency.
Conclusion
A well-structured nurse report template is an indispensable tool for healthcare professionals. It streamlines documentation, facilitates communication, and ultimately contributes to improved patient care. By understanding the purpose of each section and adhering to best practices, nurses can create templates that are both effective and efficient. The consistent application of a standardized template promotes continuity of care, reduces errors, and empowers nurses to provide the best possible care to their patients. Investing time in developing and maintaining a robust nurse report template is an investment in patient safety and operational efficiency. Nurse Report Template is a critical component of a well-functioning healthcare team.

Conclusion
The nurse report template is a cornerstone of effective patient care, streamlining documentation and facilitating communication. By understanding its core components and adhering to best practices, nurses can create templates that enhance efficiency, improve patient safety, and ultimately contribute to better outcomes. The consistent use of this template is vital for maintaining a high standard of care and ensuring that all relevant information is readily available to healthcare providers. Ultimately, a thoughtfully designed nurse report template empowers nurses to focus on what matters most: providing compassionate and effective care to their patients.