The creation and utilization of a robust Patient Care Report Template are increasingly vital for healthcare providers, administrators, and researchers. In today’s complex healthcare landscape, accurate and comprehensive data collection and reporting are essential for improving patient outcomes, streamlining workflows, and demonstrating compliance with regulatory requirements. A well-designed Template ensures consistent data capture, facilitates informed decision-making, and provides a clear audit trail. This article will delve into the key components of a successful Patient Care Report Template, exploring its purpose, structure, and best practices for effective implementation. Patient Care Report Template is more than just a document; it’s a strategic tool for optimizing patient care.
The core function of a Patient Care Report Template is to systematically document patient information, treatment plans, and clinical observations. It serves as a central repository for data, enabling healthcare professionals to quickly access critical information, identify trends, and track patient progress. Without a standardized Template, data collection can become fragmented, leading to inconsistencies and potential errors. A properly designed Template streamlines the reporting process, reducing administrative burden and freeing up valuable time for patient care. It’s a critical investment in operational efficiency and patient satisfaction. Furthermore, adherence to established Template formats and guidelines is increasingly mandated by regulatory bodies like the Health Insurance Portability and Accountability Act (HIPAA) and other compliance standards.
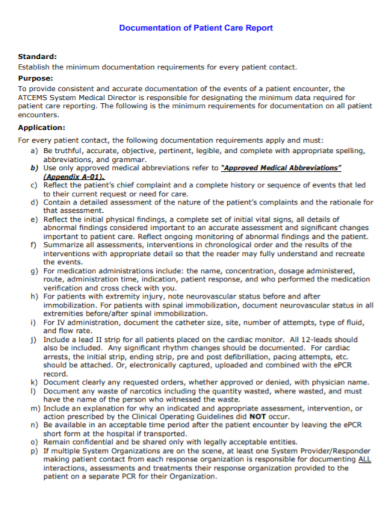
Understanding the Purpose of a Patient Care Report Template
Before diving into the specifics of the Template’s structure, it’s important to understand why it’s so crucial. The primary purpose is to provide a consolidated view of a patient’s care journey. This includes detailed information about their medical history, diagnoses, treatments, medications, and response to therapy. Beyond simply recording data, the Template facilitates communication between different healthcare providers involved in the patient’s care. It ensures that everyone has access to the same information, minimizing the risk of misunderstandings and errors. It also supports quality improvement initiatives by allowing for the identification of areas for improvement in patient care delivery. Ultimately, a well-crafted Template empowers clinicians to make informed decisions and deliver optimal patient care.
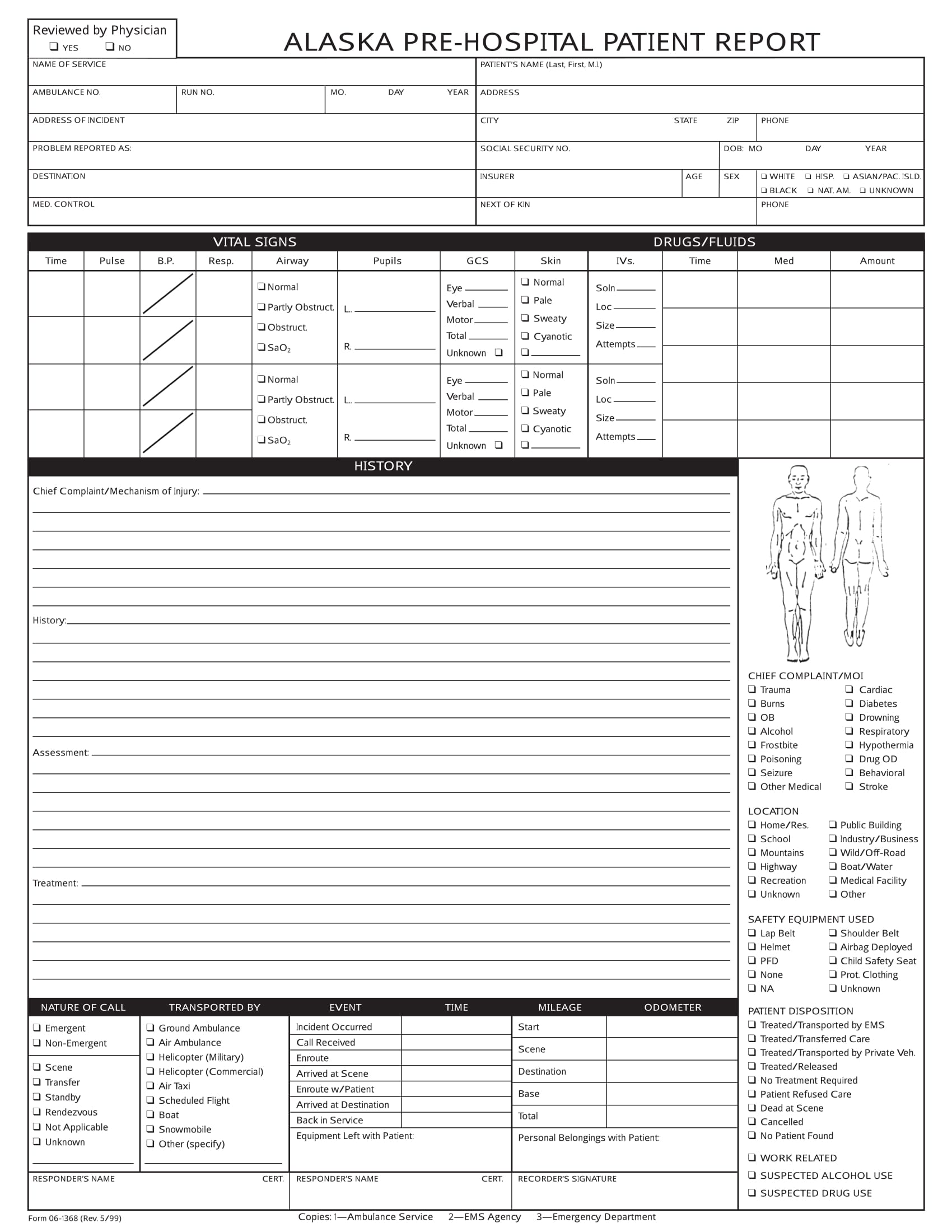
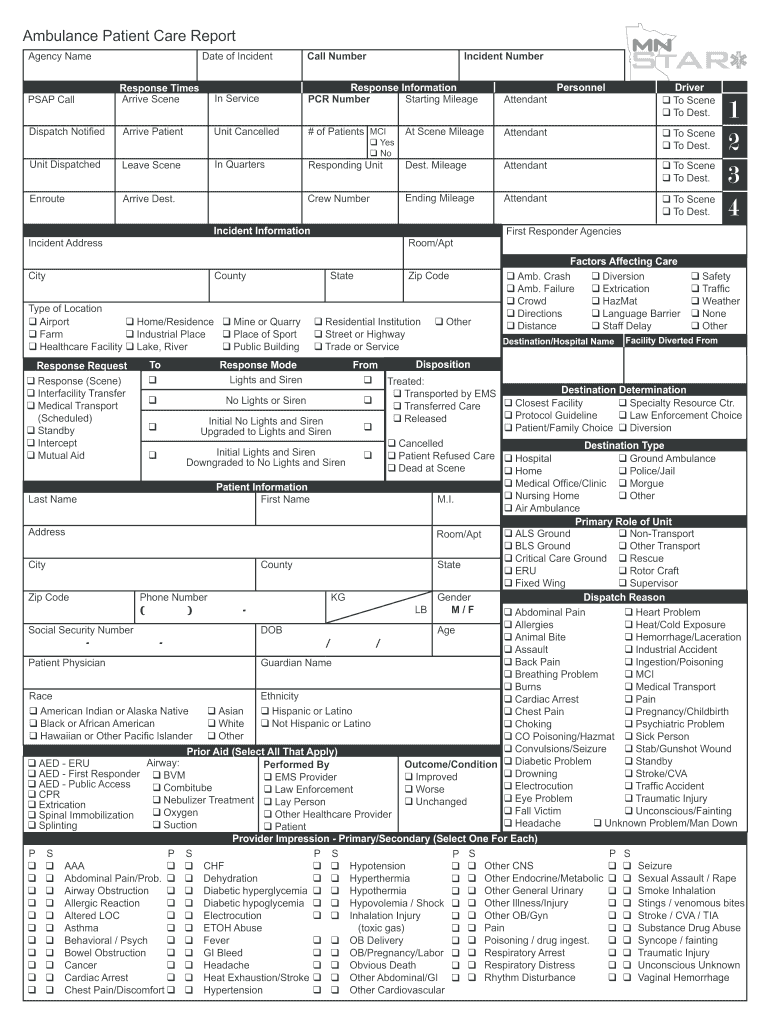
Key Sections of a Comprehensive Patient Care Report Template
Let’s examine the essential sections typically included within a Patient Care Report Template. Each section is designed to gather specific data points and provide context for the overall patient profile.
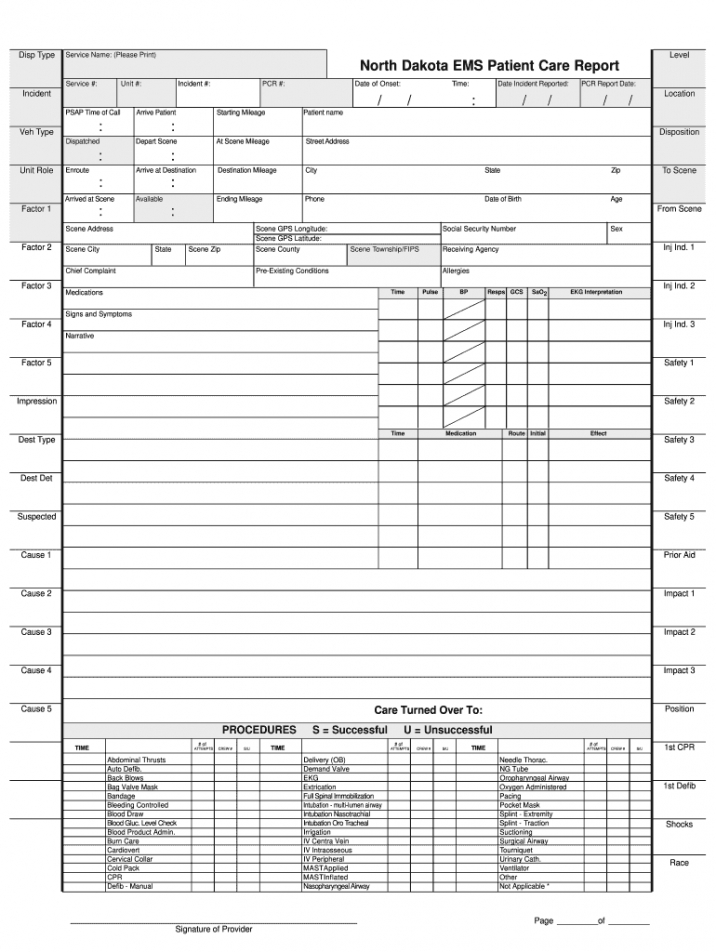
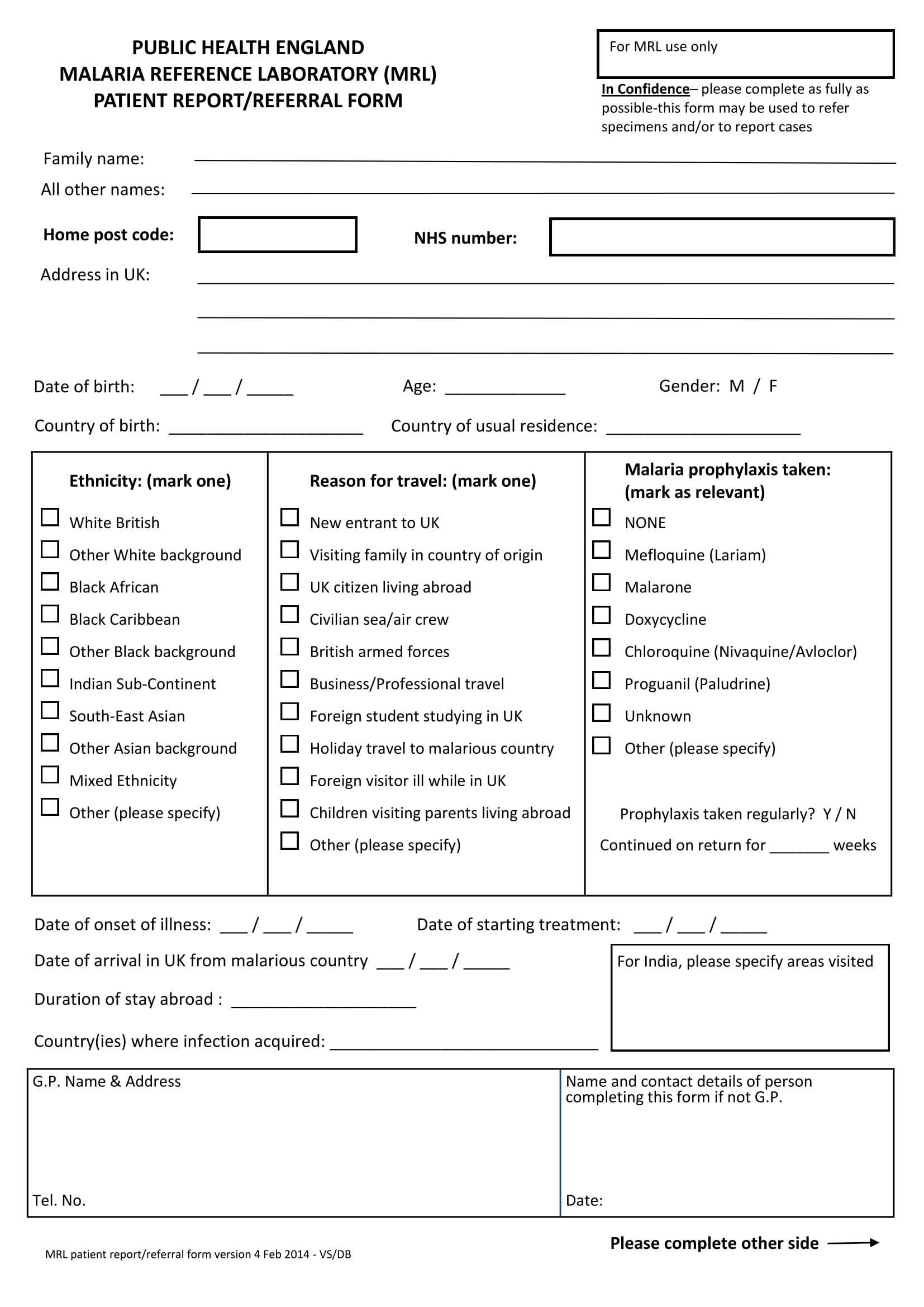
Section 1: Patient Demographics and Contact Information
This initial section gathers basic patient information, ensuring accurate identification and record-keeping. It includes the patient’s full name, date of birth, address, phone number, and email address. It’s vital to collect this information promptly and securely. Consider adding a demographic section, including age, gender, and ethnicity, for demographic analysis and population health reporting. This section is foundational for any comprehensive patient record.
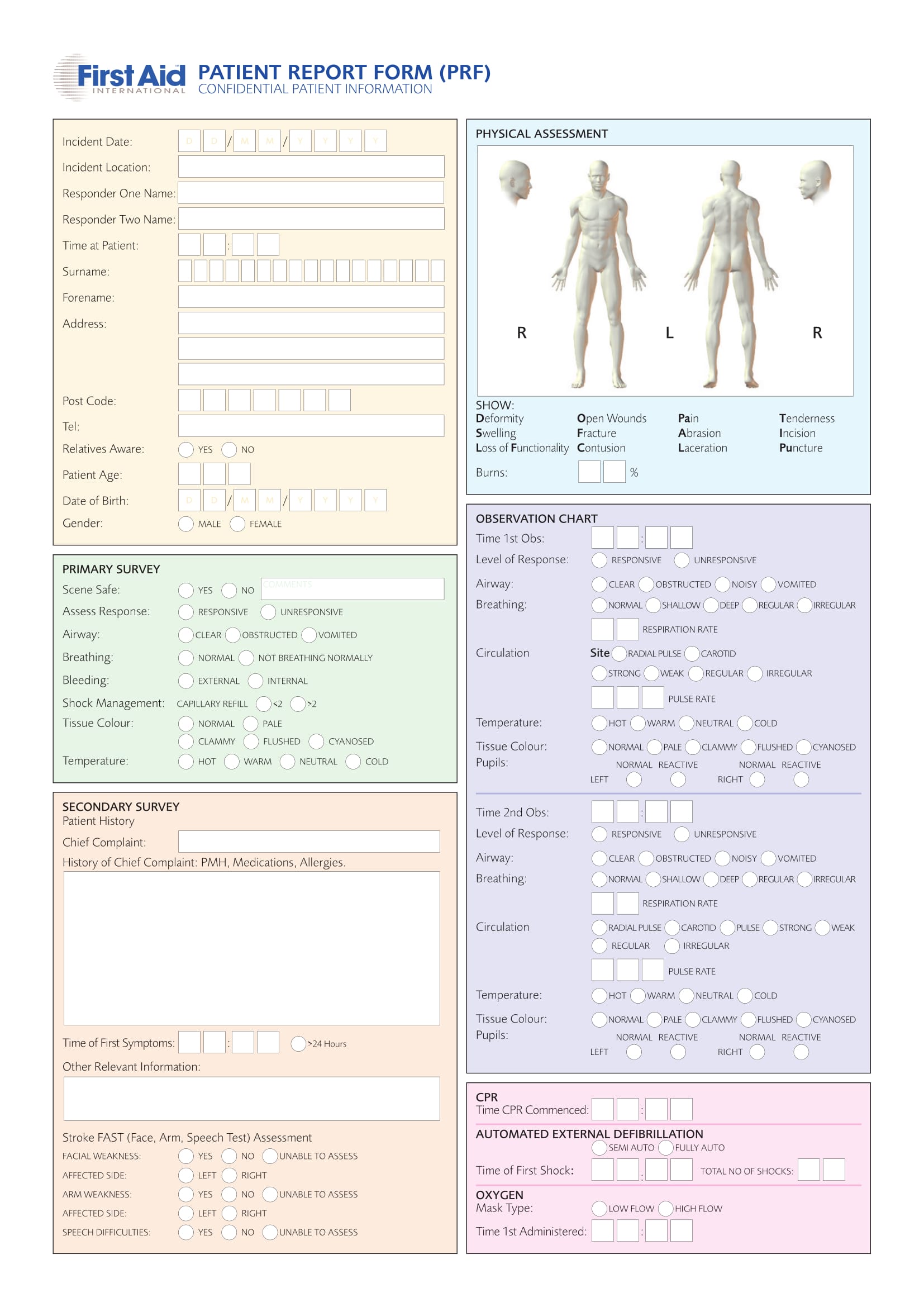
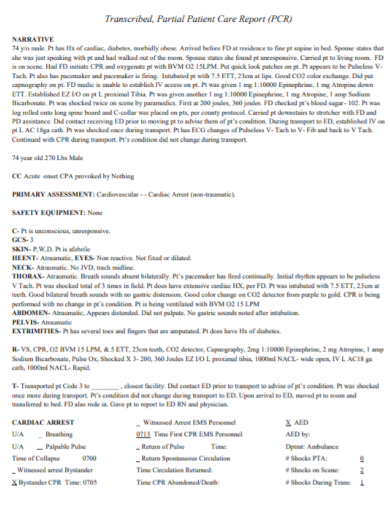
Section 2: Medical History and Background
A detailed medical history is a cornerstone of the Template. This section captures relevant information about the patient’s past illnesses, surgeries, allergies, and family history. It’s crucial to document diagnoses, treatments, and any significant medical events. The Template should include sections for documenting medication history, including dosages, frequency, and reason for administration. Furthermore, it’s important to capture information about the patient’s lifestyle, including smoking habits, alcohol consumption, and dietary habits. This holistic view of the patient’s health history is essential for personalized care.

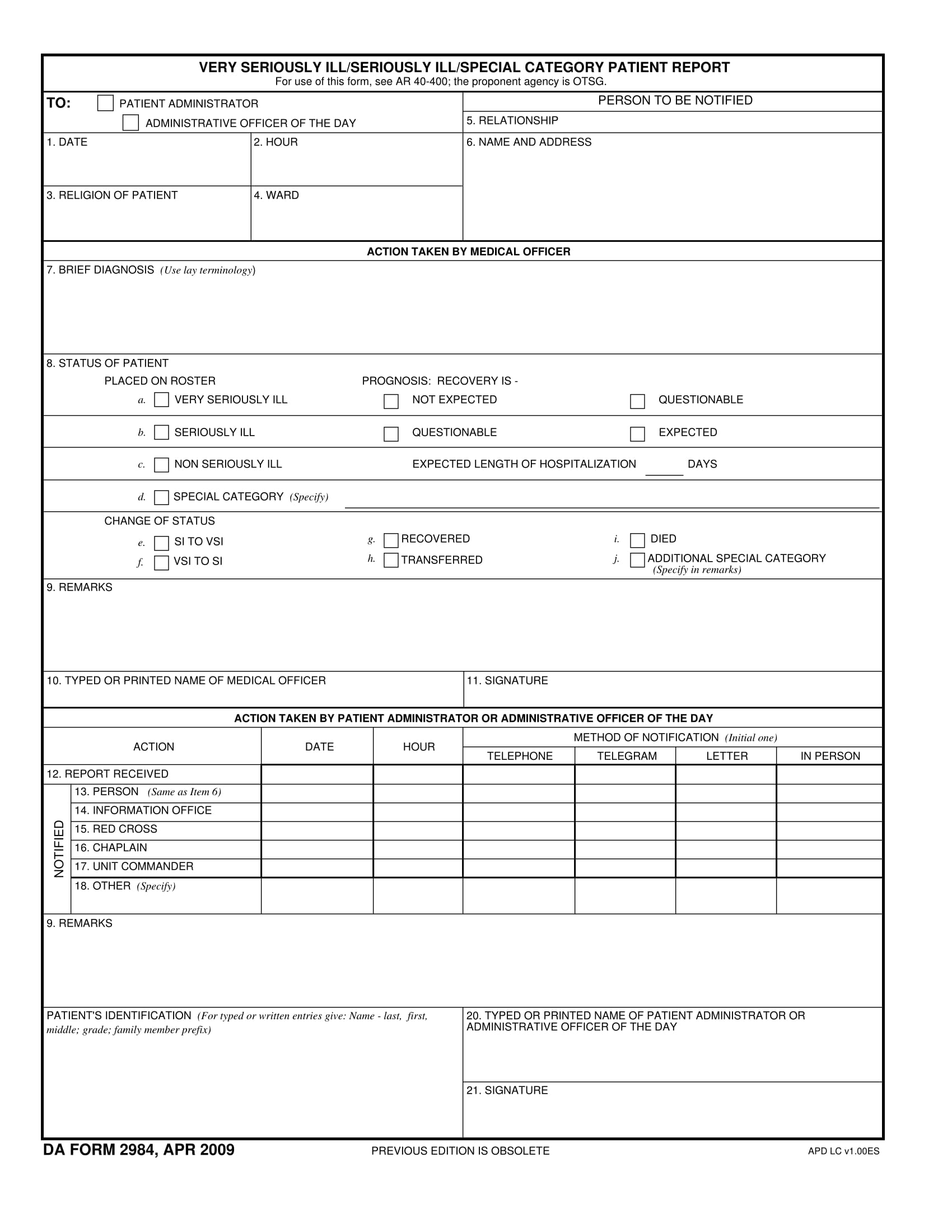
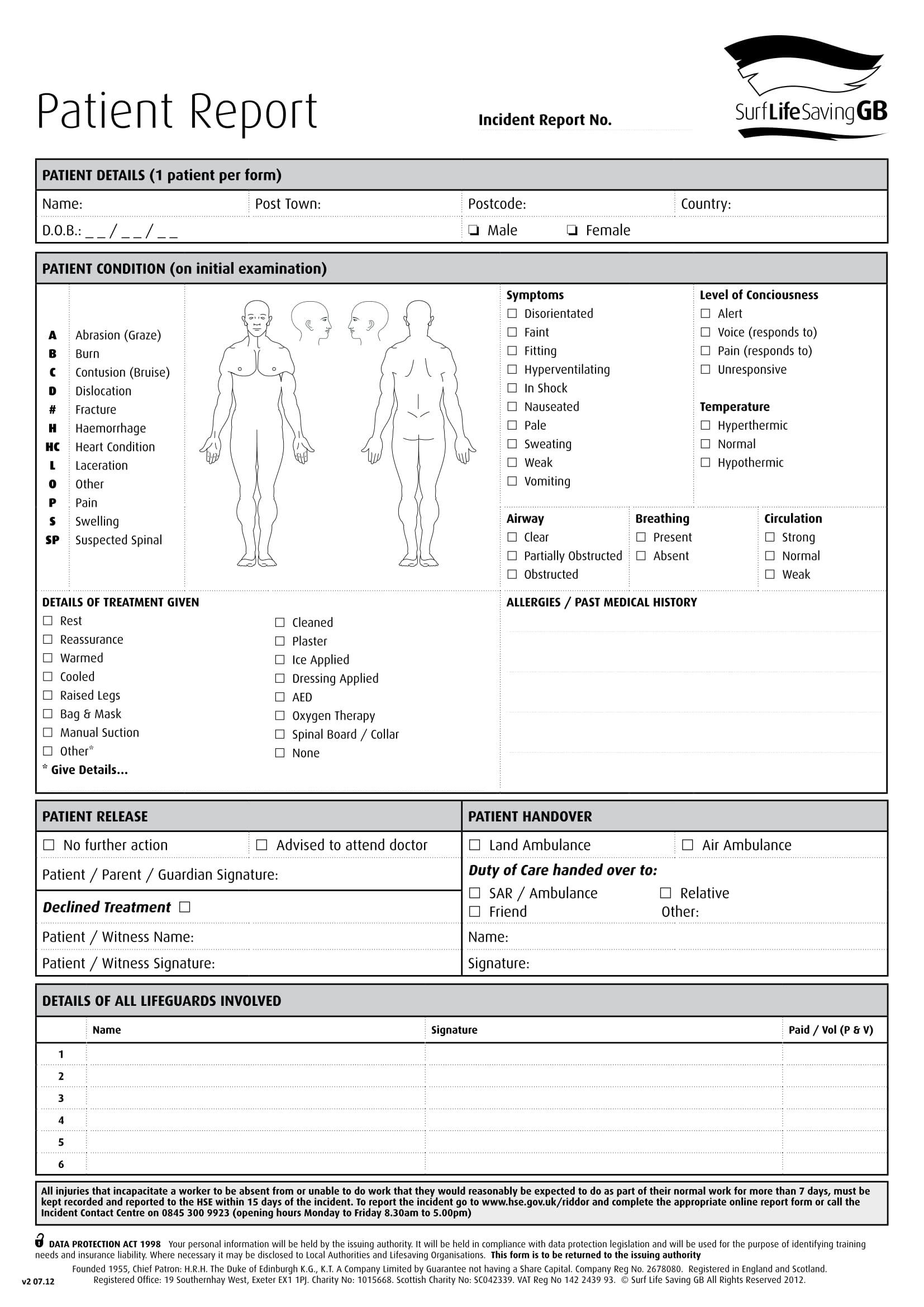
Section 3: Current Medical Condition and Diagnosis
This section focuses on the patient’s current medical condition and the underlying diagnosis. It outlines the current symptoms, physical examination findings, and laboratory results. It’s important to clearly state the diagnosis, including the ICD (International Classification of Diseases) code. The Template should also include a description of the patient’s current treatment plan, including medications, therapies, and procedures. Regular updates to this section are critical as the patient’s condition evolves.
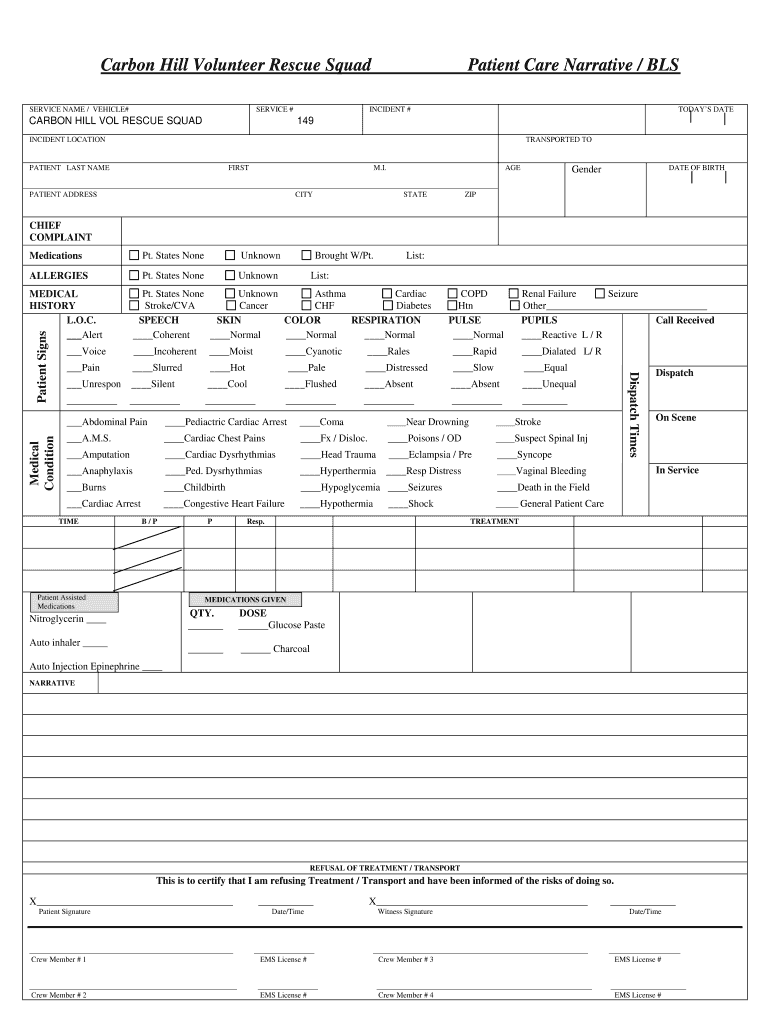
Section 4: Treatment Plan and Progress
This section details the treatment plan implemented for the patient, including the rationale for the chosen therapies and the patient’s response to treatment. It includes information on the patient’s adherence to the treatment plan, including medication adherence, appointment attendance, and follow-up visits. It also documents any adverse events or complications that have occurred during treatment. Regular monitoring and evaluation of treatment progress are essential for optimizing patient outcomes.

Section 5: Assessment and Clinical Observations
This section provides a summary of the patient’s overall clinical status, incorporating assessment findings from the medical history, physical examination, and laboratory results. It includes a description of the patient’s functional status, including their ability to perform daily activities. It also documents any changes in the patient’s condition over time. This section is particularly important for chronic disease management.
Section 6: Communication and Collaboration
This section outlines the communication and collaboration with other healthcare providers involved in the patient’s care. It includes information about consultations, referrals, and shared decision-making. It also documents the patient’s preferences regarding communication and care. Maintaining clear and consistent communication is vital for coordinated care.
Section 7: Relevant Documents and Records
This section includes links to relevant documents and records, such as lab reports, imaging studies, and physician notes. It’s important to ensure that all necessary documentation is readily accessible. This section streamlines the reporting process and reduces the need for manual data entry.
Conclusion
A well-structured and comprehensive Patient Care Report Template is an indispensable tool for healthcare providers and organizations. It streamlines data collection, facilitates communication, and supports informed decision-making. By consistently utilizing a standardized Template, healthcare professionals can improve patient outcomes, enhance operational efficiency, and demonstrate compliance with regulatory requirements. The continued evolution of technology and the increasing complexity of healthcare demand that Templates remain adaptable and reflect the changing needs of the field. Ultimately, investing in a robust Template is an investment in patient care and organizational success. Patient Care Report Template is a vital component of a patient-centered approach to healthcare.
Conclusion
The Patient Care Report Template represents a fundamental element of modern healthcare administration. Its multifaceted nature – encompassing detailed patient demographics, comprehensive medical history, and meticulous treatment plans – underscores its critical role in delivering quality, coordinated, and patient-focused care. The template’s adaptability, facilitated by digital platforms and streamlined data entry, further enhances its value. As healthcare continues to evolve, the importance of a reliable and effective Patient Care Report Template will only continue to grow, solidifying its position as a cornerstone of effective healthcare delivery. The consistent application of this template contributes significantly to improved patient outcomes and a more efficient healthcare system.