The world of mental health care increasingly relies on a structured and documented approach to patient care. One such approach is the Soap Notes Counseling Template, a system designed to capture detailed information about a client’s session, facilitating continuity of care and providing valuable insights for therapists and other professionals. This template isn’t just a collection of notes; it’s a tool for building a comprehensive understanding of the client’s experience and needs. Soap Notes Counseling Template is becoming a standard practice in many therapeutic settings, offering a significant advantage in terms of patient outcomes and professional efficiency. It’s a shift towards a more holistic and client-centered approach to therapy. Understanding the principles behind this template and its benefits is crucial for anyone involved in providing mental health services. This article will delve into the structure, purpose, and practical applications of the Soap Notes Counseling Template, providing you with the knowledge to effectively utilize it in your practice.
Understanding the Core Principles
At its heart, the Soap Notes Counseling Template is built on the principle of detailed documentation. It moves beyond simply recording what the client says to capturing the how and why behind their experiences. This includes observations about the client’s behavior, emotional state, thoughts, and any relevant contextual factors. The template encourages therapists to consider the client’s history, current stressors, and overall well-being when interpreting the session notes. It’s about moving beyond a superficial account of a session to a richer, more nuanced understanding. The template’s design prioritizes clarity and conciseness, ensuring that the information is easily accessible and understandable for both the therapist and the client. Effective use of the template requires a commitment to thoroughness and a focus on the client’s perspective.
The Template Structure: A Step-by-Step Guide
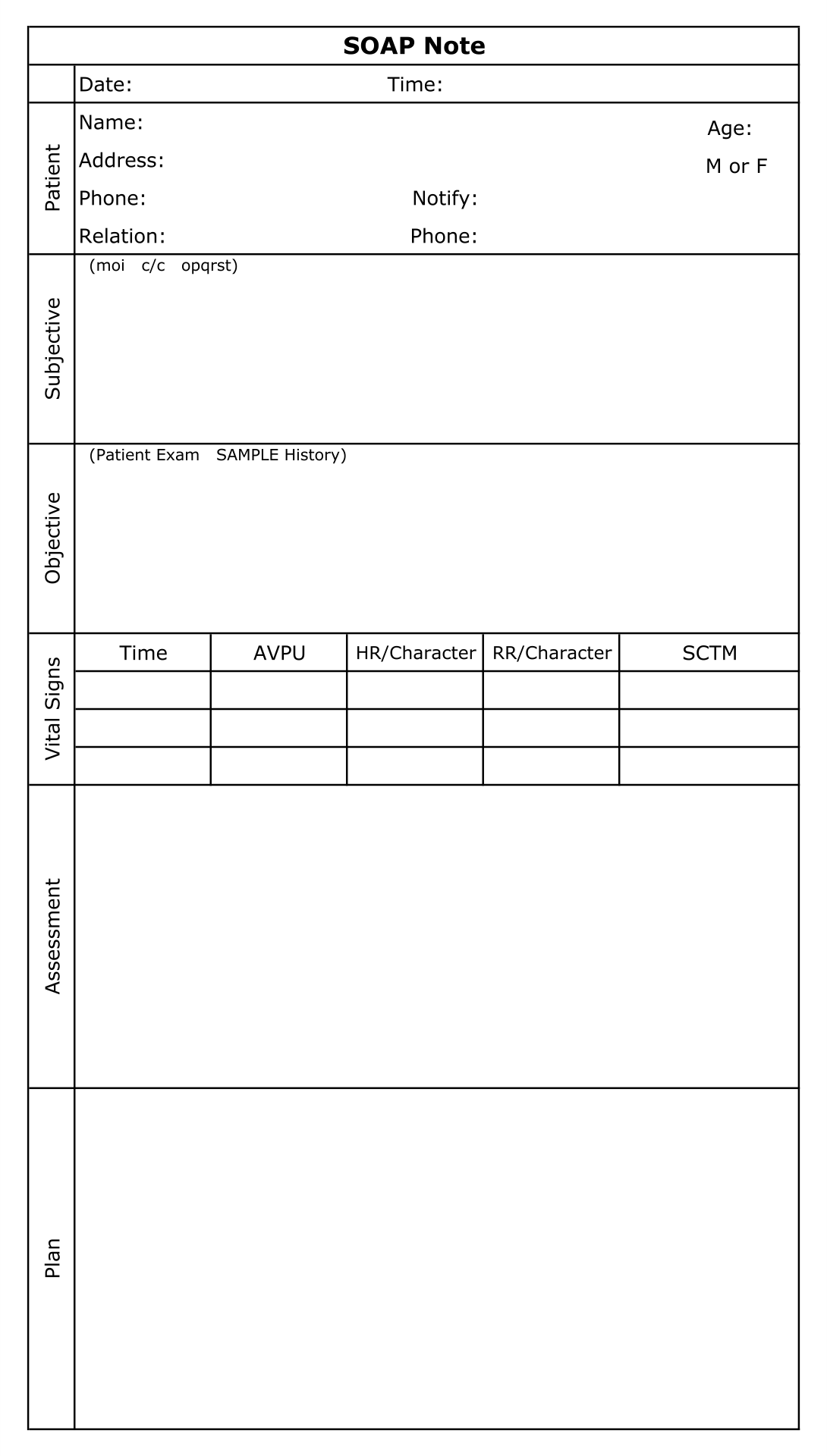
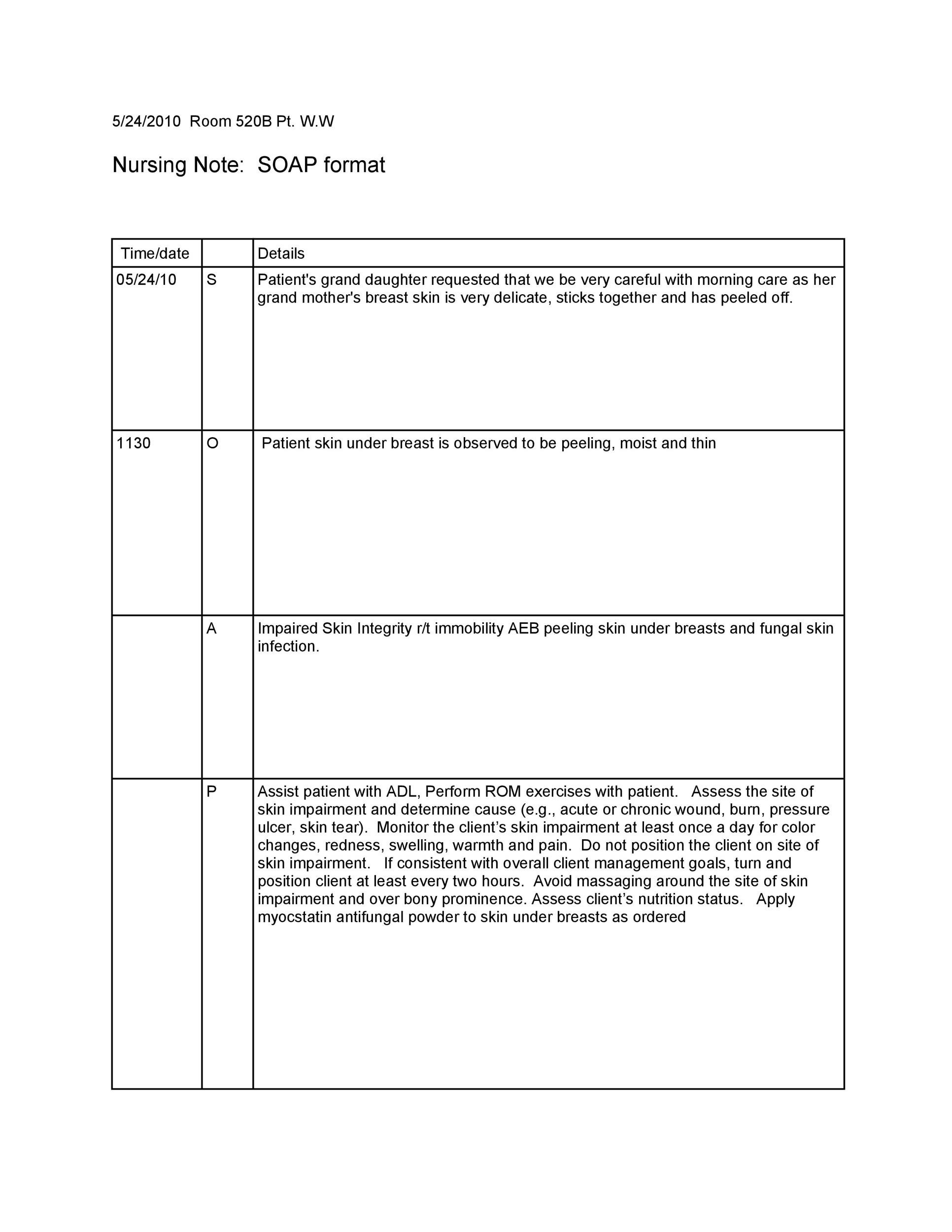
The Soap Notes Counseling Template is typically structured in a way that facilitates easy retrieval and analysis. It generally includes the following sections:

- Client Information: This section gathers essential details about the client, including demographics, contact information, and any relevant medical history.
- Session Summary: A brief overview of the session’s purpose, goals, and any key events or discussions.
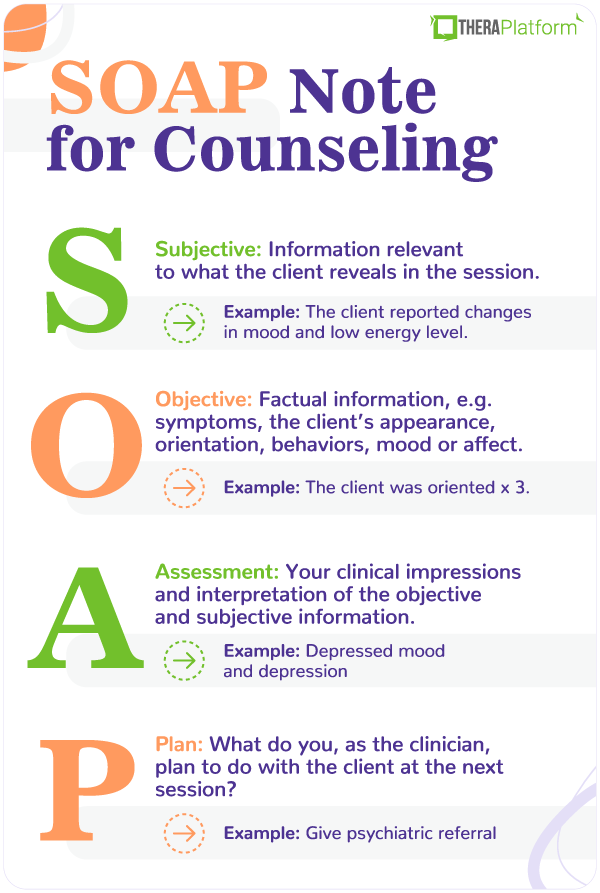
- Client’s Verbal Report: This is the core of the template, containing a detailed account of what the client said, including their language, tone, and any relevant emotional expressions.
- Client’s Non-Verbal Report: This section captures observations about the client’s body language, facial expressions, and other non-verbal cues.
- Therapist’s Observations: This is where the therapist’s interpretation and assessment of the session take place. It includes detailed notes on the client’s behavior, thoughts, feelings, and any relevant contextual factors.
- Plan of Action: A clear and specific plan outlining the next steps for the client, based on the session’s content and goals.
- Client’s Feedback: A space for the client to provide their own feedback on the session, including their thoughts, feelings, and any concerns they may have.
Section 1: Detailed Client Information – Building a Foundation
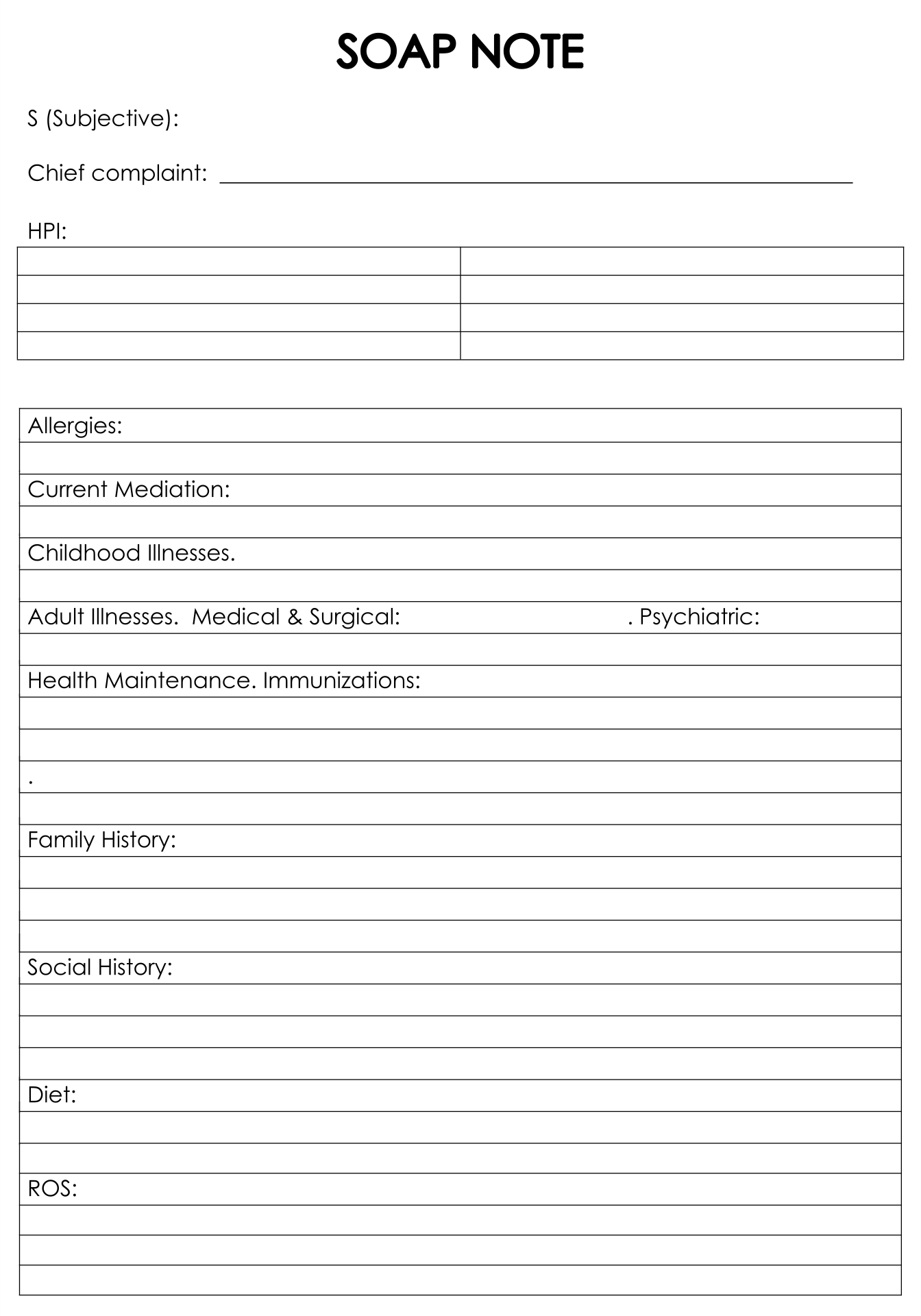
The initial section of the template is critical for establishing a solid foundation for the entire session. It’s essential to gather accurate and complete information about the client. This includes:
- Demographics: Name, age, gender, contact information, and any relevant insurance details.
- Presenting Problem/Reason for Session: A clear and concise description of the client’s primary concerns or issues. This is a crucial element for tailoring the therapeutic approach.
- Medical History: Any relevant medical conditions, medications, allergies, or past surgeries. This section requires careful consideration of privacy and confidentiality.
- Psychiatric History: Previous diagnoses, treatment history, and any significant past episodes of mental health challenges.
- Social History: Information about the client’s family, relationships, living situation, and social support system. This helps understand the context of their challenges.
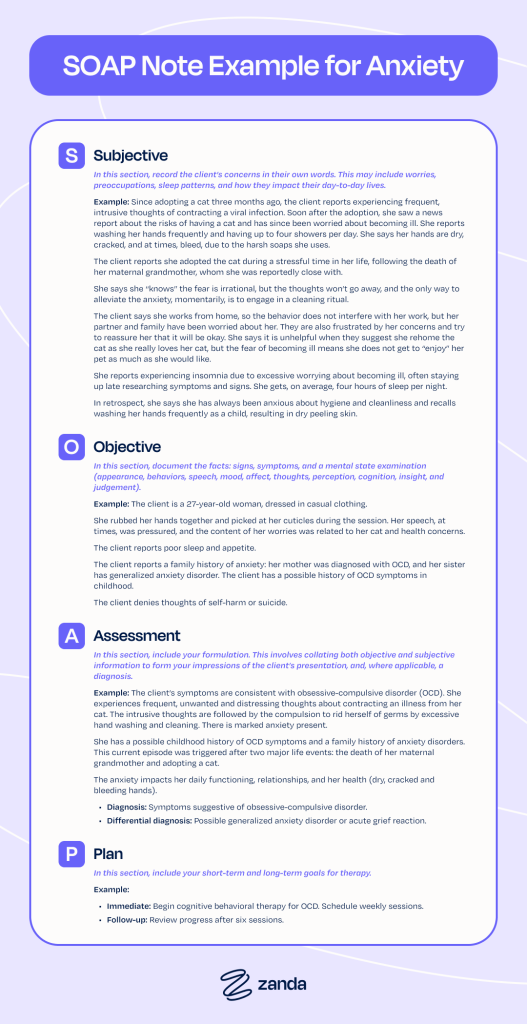
Section 2: Client’s Verbal Report – Unpacking the Narrative
This section is arguably the most important, as it provides the raw material for the therapist’s interpretation. It’s not about simply transcribing what the client says; it’s about understanding how they say it.
- Language and Tone: Note the client’s word choice, sentence structure, and overall tone. Are they using formal or informal language? Are they expressing themselves clearly or hesitantly?
- Emotional Expression: Identify the client’s emotional state – anxiety, sadness, anger, joy, etc. Pay attention to the intensity and duration of these emotions.
- Key Themes and Ideas: What are the central themes or ideas that the client is expressing? Look for recurring patterns or topics.
- Specific Examples: Quote directly from the client’s words to illustrate their points. This adds credibility and helps the therapist understand the client’s perspective.
- Challenges and Resistance: Note any challenges the client presents, such as resistance to discussing certain topics or difficulty articulating their feelings.
Soap Notes Counseling Template – Understanding the Client’s Perspective
This section is specifically designed to capture the client’s perspective. It’s a space for the therapist to actively listen and reflect on the client’s words. The therapist should ask clarifying questions to ensure they fully understand the client’s experience. For example, “Can you tell me more about what you mean by…?” or “What does that feel like for you?”

Section 3: Non-Verbal Observations – Beyond the Words
Often, what a client doesn’t say is just as important as what they do say. Non-verbal cues can provide valuable insights into their emotional state and experiences.
- Body Language: Observe posture, gestures, facial expressions, and eye contact. Are they open and engaged, or closed off and withdrawn?
- Facial Expressions: Note any expressions of emotion – smiles, frowns, raised eyebrows, etc.
- Tone of Voice: Pay attention to the pitch, volume, and rhythm of the client’s voice. Are they speaking quickly or slowly? Are they using a calm or agitated tone?
- Gestures: Observe any hand movements or other gestures that may be associated with their emotions or thoughts.
Section 4: Therapist’s Observations – The Art of Interpretation
This section is where the therapist’s expertise and clinical judgment come into play. It’s not about simply recording observations; it’s about interpreting them and drawing conclusions.
- Behavioral Analysis: Analyze the client’s behavior in relation to their verbal report and non-verbal cues. Are there any patterns or themes that emerge?
- Thought Processes: Identify the client’s thoughts and beliefs, and how they relate to their experiences.
- Emotional Regulation: Assess the client’s ability to regulate their emotions. Are they experiencing any distress or anxiety?
- Contextual Factors: Consider any contextual factors that may be influencing the client’s behavior or experience – stressors, relationships, or social support.
Section 5: Plan of Action – Moving Forward
The Plan of Action is a crucial element of the Soap Notes Counseling Template. It outlines the specific steps that will be taken to address the client’s needs and goals.
- Specific Goals: Clearly define the client’s goals for therapy.
- Treatment Modalities: Specify the therapeutic interventions that will be used – e.g., cognitive behavioral therapy, mindfulness, etc.
- Homework Assignments: Assign any homework assignments that the client will be expected to complete.
- Follow-Up Schedule: Establish a schedule for follow-up appointments.
Conclusion
The Soap Notes Counseling Template is a powerful tool for facilitating effective therapy. By providing a structured and detailed framework for documenting client sessions, it allows therapists to gain a deeper understanding of their clients’ experiences and needs. The template’s emphasis on thoroughness, clarity, and client-centeredness makes it a valuable asset for anyone involved in providing mental health services. Ultimately, the effectiveness of the template hinges on the therapist’s ability to accurately and thoughtfully interpret the information it contains. Consistent and thoughtful application of the template will undoubtedly lead to improved patient outcomes and a more holistic approach to care. Remember that the template is a tool, and its success depends on the therapist’s skill and judgment.
Conclusion
The Soap Notes Counseling Template represents a significant advancement in therapeutic practice, moving beyond a simple record-keeping system to a dynamic tool for understanding and addressing the complexities of the human experience. Its structured approach, coupled with the emphasis on detailed observation and thoughtful interpretation, empowers therapists to build stronger therapeutic relationships and deliver more effective care. The continued evolution of this template, incorporating technological advancements and incorporating client-centered principles, promises to further refine its utility and impact on the field of mental health. The core principles of thoroughness, clarity, and client-centeredness remain paramount, ensuring that the template remains a valuable asset for years to come.