The efficient and accurate creation of medical office notes is paramount to providing excellent patient care and ensuring seamless communication between healthcare providers. A well-structured medical office note template serves as a crucial tool for documenting patient encounters, tracking progress, and facilitating continuity of care. This article will explore the essential components of a robust medical office note template, offering practical guidance for healthcare professionals looking to optimize their documentation practices. Medical Office Note Template – understanding its purpose and utilizing it effectively is a significant investment in patient satisfaction and operational efficiency. This guide will delve into the key elements, best practices, and potential variations to ensure your notes are clear, concise, and compliant with relevant regulations.
What is a Medical Office Note Template?
A medical office note template is a standardized format for recording patient interactions. It’s more than just a simple checklist; it’s a structured framework designed to capture essential information, ensuring consistency and facilitating easy retrieval of patient history. The purpose is to streamline the note-taking process, reducing errors, and improving the overall quality of care. Different healthcare settings and specialties may utilize slightly different templates, but the core principles remain consistent. A thoughtfully designed template allows providers to quickly and accurately document vital details, contributing to a comprehensive and organized patient record. The benefits extend beyond simple documentation; it fosters accountability, improves communication, and ultimately enhances the patient experience.
Core Components of a Medical Office Note Template
A comprehensive medical office note template typically includes several key sections. Each section is designed to address a specific aspect of the patient encounter. Let’s examine some of the most important components:

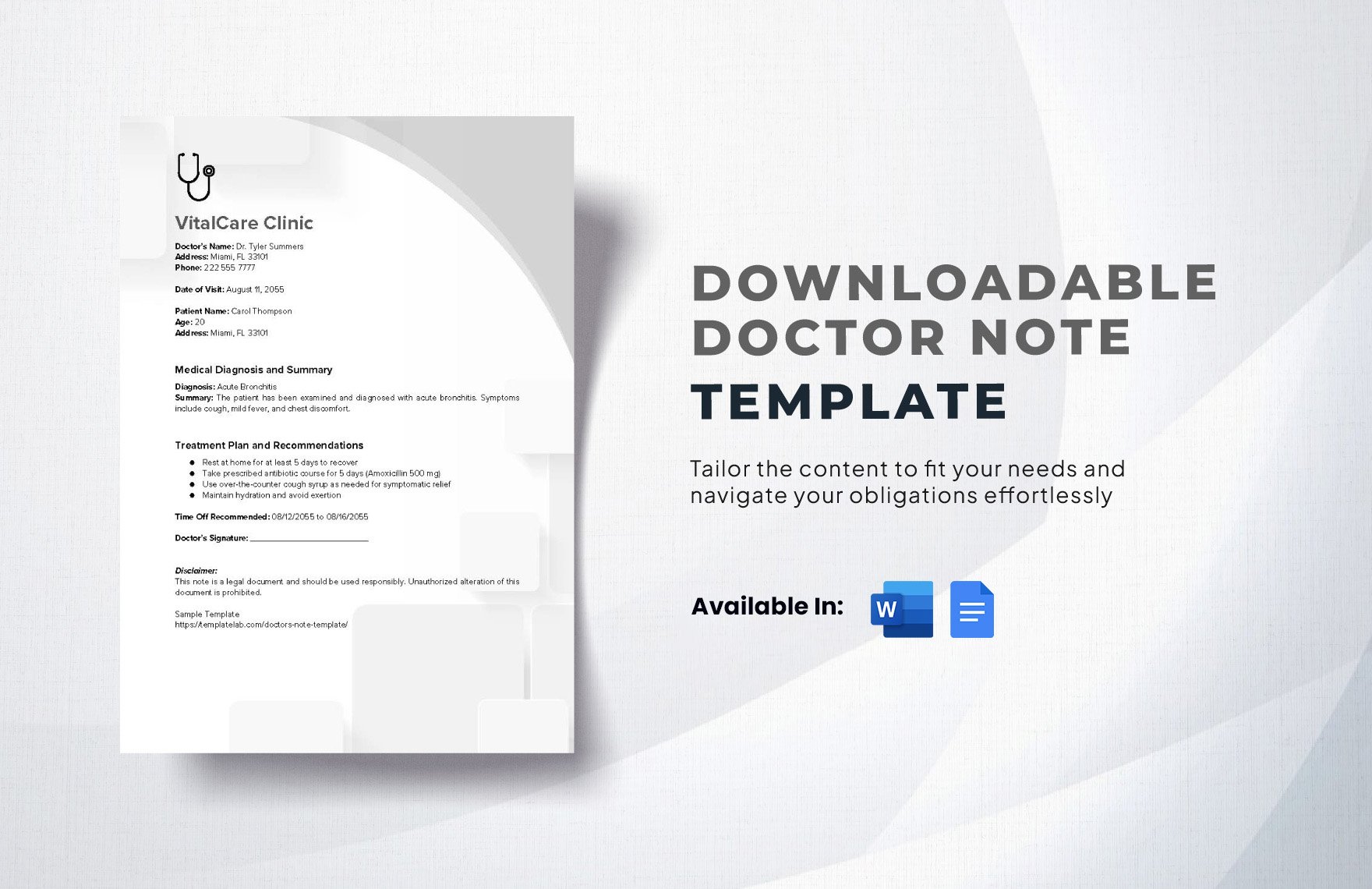
Section 1: Patient Demographics & Initial Contact
This section gathers basic information about the patient, ensuring a complete record. It typically includes:
- Patient Name: Clearly and accurately recorded.
- Date of Birth: Essential for accurate record-keeping.
- Medical Record Number (MRN): A unique identifier for the patient’s record.
- Contact Information: Phone number and email address for follow-up.
- Referring Physician (if applicable): Information about the provider who referred the patient.
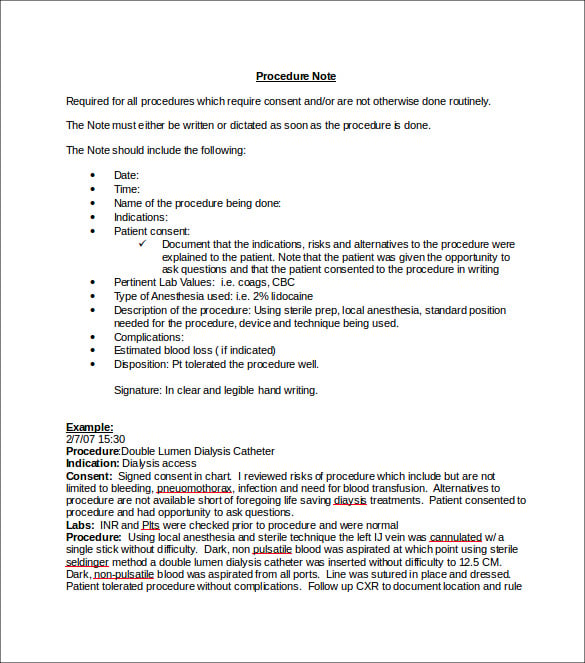
Section 2: Encounter Summary
This is the heart of the note, providing a concise overview of the patient’s visit. It should include:
- Date and Time of Encounter: Critical for tracking trends and identifying patterns.
- Reason for Visit: A brief description of the patient’s primary concern.
- Chief Complaint: The patient’s primary reason for seeking medical attention.
- History of Present Illness (HPI): A detailed account of the patient’s current symptoms and their progression.
- Relevant History: Past medical history, surgical history, allergies, and medications.
Section 3: Physical Examination Findings
This section details the observations made during the physical examination. It should include:
- Vital Signs: Temperature, blood pressure, heart rate, respiratory rate, and oxygen saturation.
- Observations: Detailed descriptions of any abnormalities observed, such as skin changes, swelling, or tenderness.
- Diagnostic Tests: Results of any laboratory tests, imaging studies, or other diagnostic procedures.
Section 4: Assessment & Plan
This section outlines the healthcare provider’s assessment of the patient’s condition and the proposed plan of care. It should include:

- Diagnosis: The final diagnosis or suspected diagnosis.
- Treatment Plan: Specific recommendations for treatment, including medications, therapies, and lifestyle modifications.
- Prognosis: An estimated outcome of the patient’s condition.
Section 5: Documentation of Communication & Education
This section captures any communication with the patient and any education provided. It includes:
- Patient Education: Information provided to the patient about their condition, treatment, and follow-up care.
- Shared Decision-Making: Discussion of the patient’s preferences and goals.
- Medication Reconciliation: A summary of the patient’s current medications and dosages.
Utilizing “Medical Office Note Template” Effectively
The effectiveness of a medical office note template hinges on its clarity and completeness. Medical Office Note Template – it’s not enough to simply fill in the sections; each element must be accurate, objective, and relevant to the patient’s situation. Consider these tips:
- Be Concise: Use clear and concise language. Avoid jargon and unnecessary details.
- Be Specific: Provide specific details rather than vague descriptions.
- Objectivity: Maintain an objective tone and avoid personal opinions.
- Accuracy: Double-check all information for accuracy.
- Consistency: Use consistent terminology and formatting throughout the note.
The Importance of Compliance and Regulations
Healthcare providers must adhere to strict regulations regarding patient documentation, such as HIPAA (Health Insurance Portability and Accountability Act). These regulations dictate how patient information can be collected, stored, and shared. Maintaining accurate and compliant medical office notes is crucial for protecting patient privacy and ensuring legal compliance. Furthermore, many insurance companies require specific documentation standards, which can influence the format and content of medical notes. Staying informed about these regulations is essential for maintaining a professional and compliant practice.
Conclusion
Medical office note templates are indispensable tools for healthcare professionals, streamlining documentation, improving patient care, and ensuring regulatory compliance. By understanding the core components of a well-structured template and utilizing it effectively, providers can significantly enhance their practice efficiency and contribute to a more patient-centered approach to healthcare. The continued evolution of electronic health records (EHRs) and digital documentation tools necessitates a commitment to maintaining a robust and adaptable template system. Investing in training and ensuring consistent application of the template are key to maximizing its benefits. Ultimately, a thoughtfully designed and consistently utilized medical office note template is a cornerstone of quality patient care.
Conclusion
The meticulous and strategic application of a medical office note template represents a fundamental pillar of effective healthcare delivery. From facilitating seamless communication between providers to ensuring accurate record-keeping, this standardized approach significantly enhances patient safety and operational efficiency. Continued refinement and adaptation to evolving regulatory landscapes will undoubtedly solidify its position as an indispensable tool within the healthcare ecosystem. The consistent utilization of this template fosters a culture of transparency and accountability, ultimately benefiting both patients and practitioners alike.