The healthcare landscape is constantly evolving, demanding efficient and organized documentation for pediatric care. A well-structured pediatric soap note is no longer a luxury – it’s a critical component of patient safety, continuity of care, and billing accuracy. This article will delve into the essential elements of a robust pediatric soap note template, providing you with the knowledge to create and utilize these vital documents effectively. Pediatric Soap Note Template – understanding its purpose and how to create it is paramount for any healthcare professional working with children. This guide will cover everything from the core sections to best practices for formatting and ensuring clarity.
Understanding the Importance of Pediatric Soap Notes
Before we dive into the specifics, it’s crucial to understand why pediatric soap notes are so important. They serve as a concise record of a patient’s encounter, capturing key information quickly and efficiently. This allows for seamless transitions between providers, reduces errors, and facilitates accurate billing. Without a standardized format, clinicians risk losing valuable details, leading to potential complications and increased administrative burden. Furthermore, a well-maintained soap note contributes to improved patient safety by providing a clear history of the care provided. The ability to quickly access and review a patient’s history is vital, especially in situations requiring immediate intervention. The consistent use of a standardized template ensures all relevant information is captured, minimizing the risk of missing crucial details. Ultimately, a thoughtfully designed pediatric soap note streamlines workflows and enhances the quality of patient care.

Core Sections of a Pediatric Soap Note
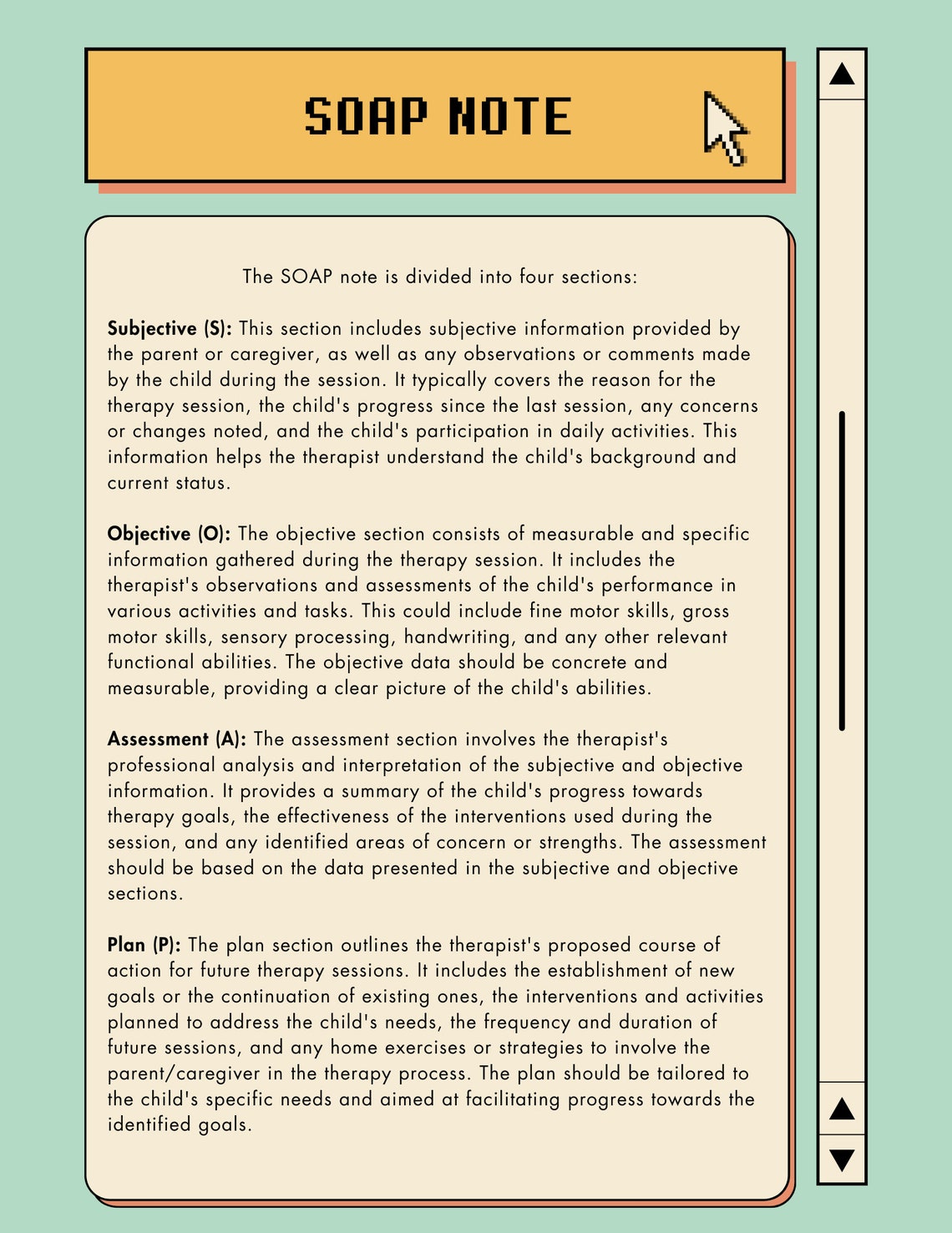
A comprehensive pediatric soap note typically includes several key sections. Each section is designed to gather specific information relevant to the patient’s condition and treatment. Here’s a breakdown of the essential components:
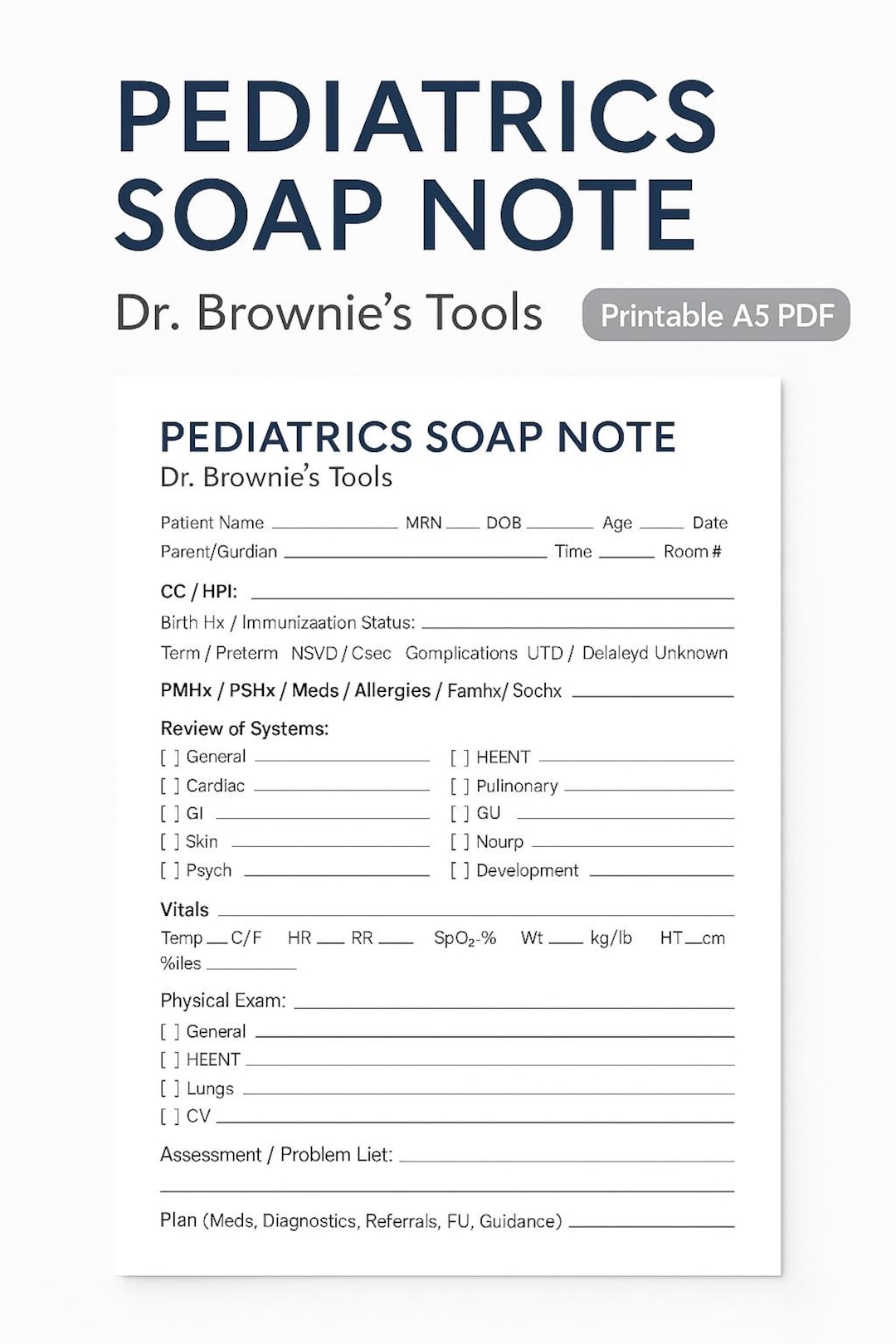
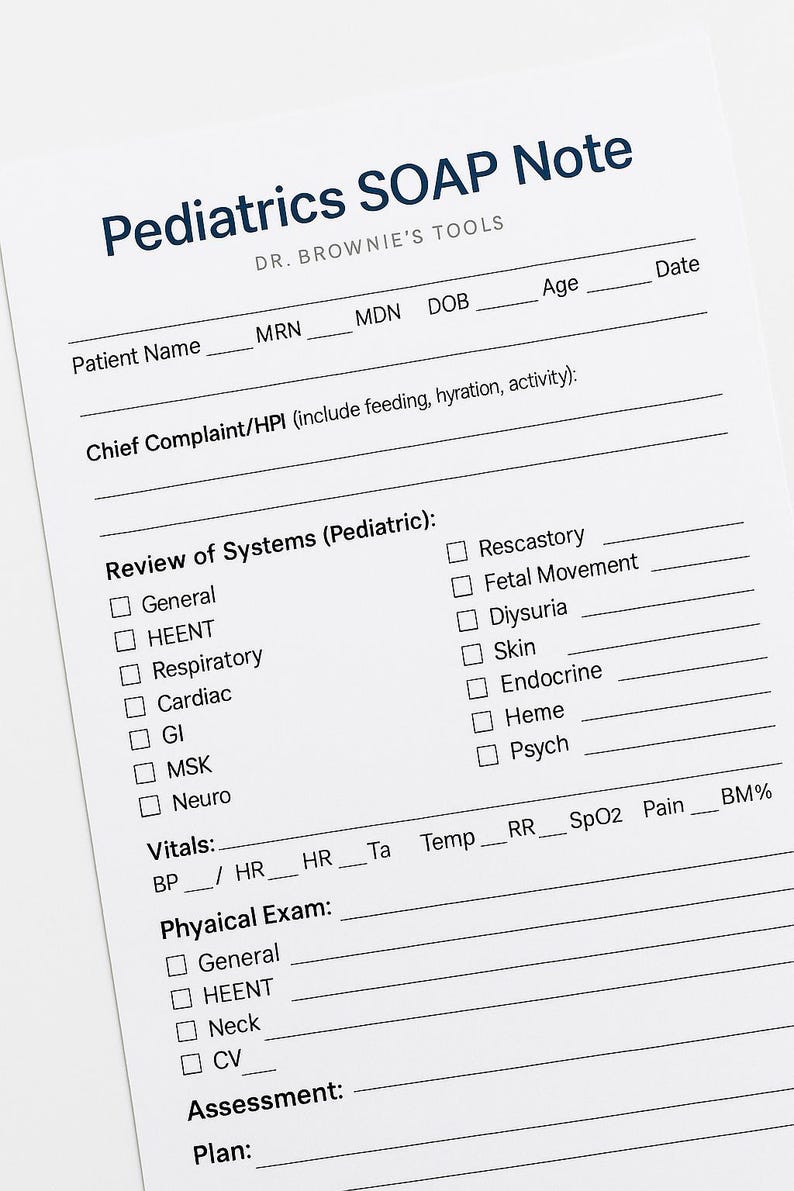
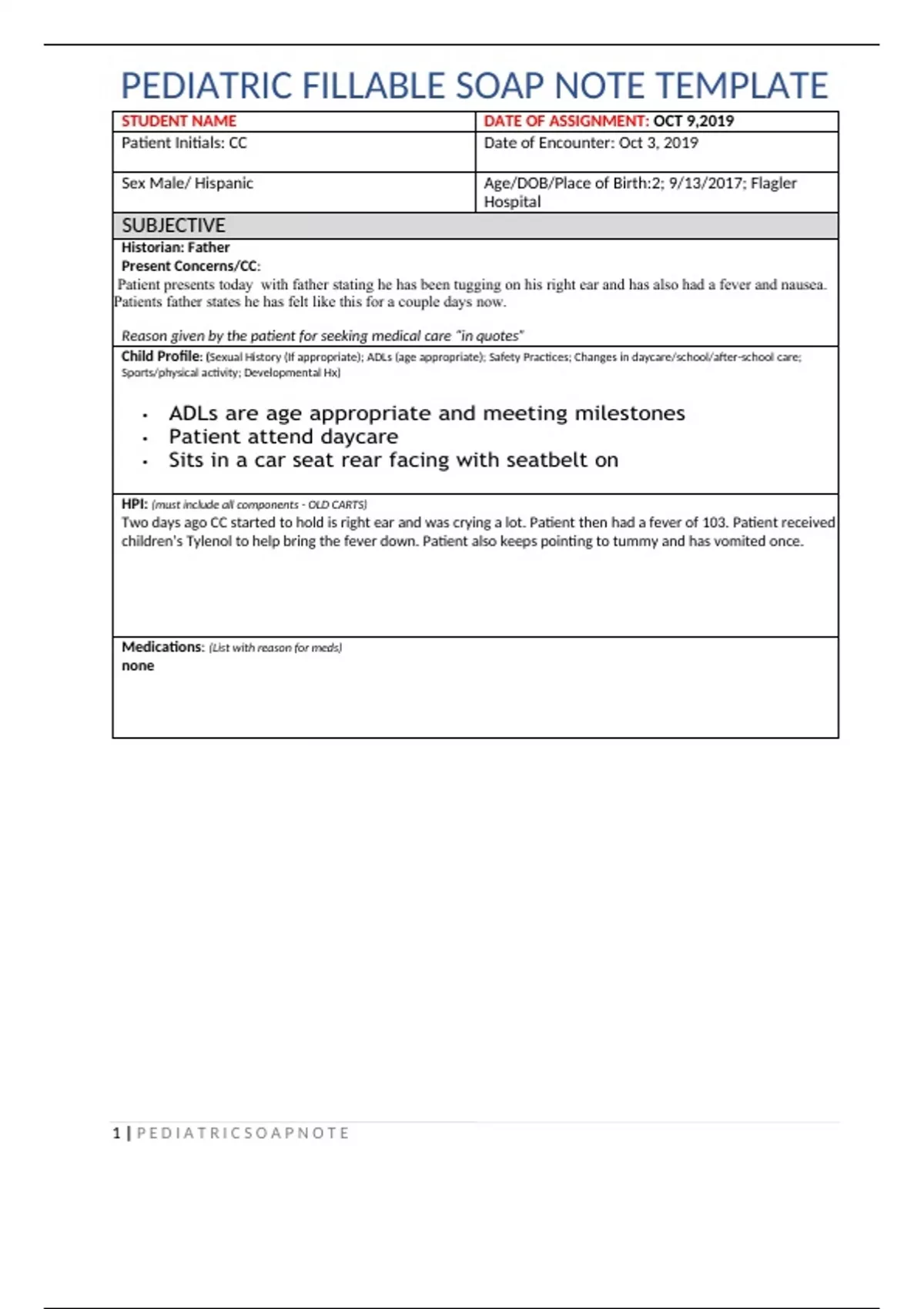
1. Patient Demographics
This section provides basic information about the patient, ensuring easy identification and tracking. It includes:
- Patient Name: Full name, including any nicknames.
- Date of Birth: Crucial for age-related considerations.
- Medical Record Number (MRN): Essential for accurate identification.
- Contact Information: Phone number, address, and emergency contact details.
- Insurance Information: Policy number and group name.
2. Chief Complaint
This section clearly states the reason for the patient’s visit. It’s a concise and direct statement of the primary concern.

- Example: “Patient presents with fever, cough, and difficulty breathing.”
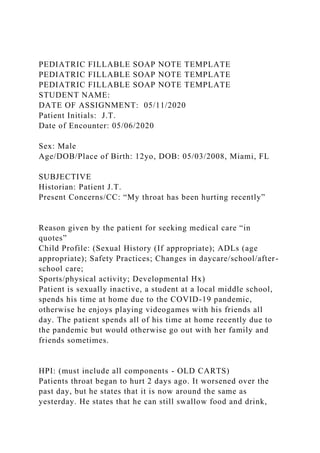
3. History of Present Illness (HPI)
This is arguably the most important section, detailing the patient’s current symptoms and their progression. It’s a narrative account of the patient’s experience.
- Detailed Description: Expand on the chief complaint, including onset, duration, severity, and any aggravating or alleviating factors.
- Associated Symptoms: Include any other symptoms the patient is experiencing (e.g., rash, pain, nausea).
- Past Medical History: Briefly outline relevant past illnesses, surgeries, and hospitalizations.
- Medications: List all current medications, including dosage and frequency.
4. Physical Examination
This section describes the findings from the physical examination. It’s a systematic and objective assessment of the patient’s physical condition.
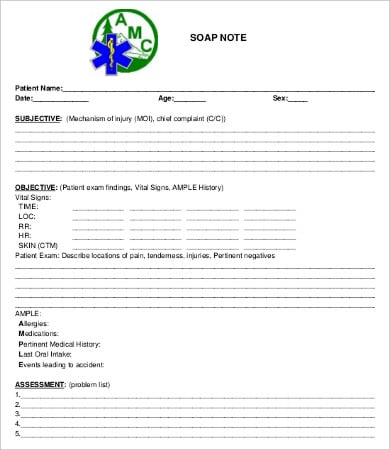
- Vital Signs: Temperature, pulse, respiration rate, blood pressure, and oxygen saturation.
- Head and Neck: Assess for signs of infection (e.g., nasal discharge, throat redness).
- Musculoskeletal: Observe for any abnormalities in the joints or muscles.
- Skin: Note any rashes, lesions, or other skin changes.
- Neurological: Assess reflexes, sensation, and cranial nerves.
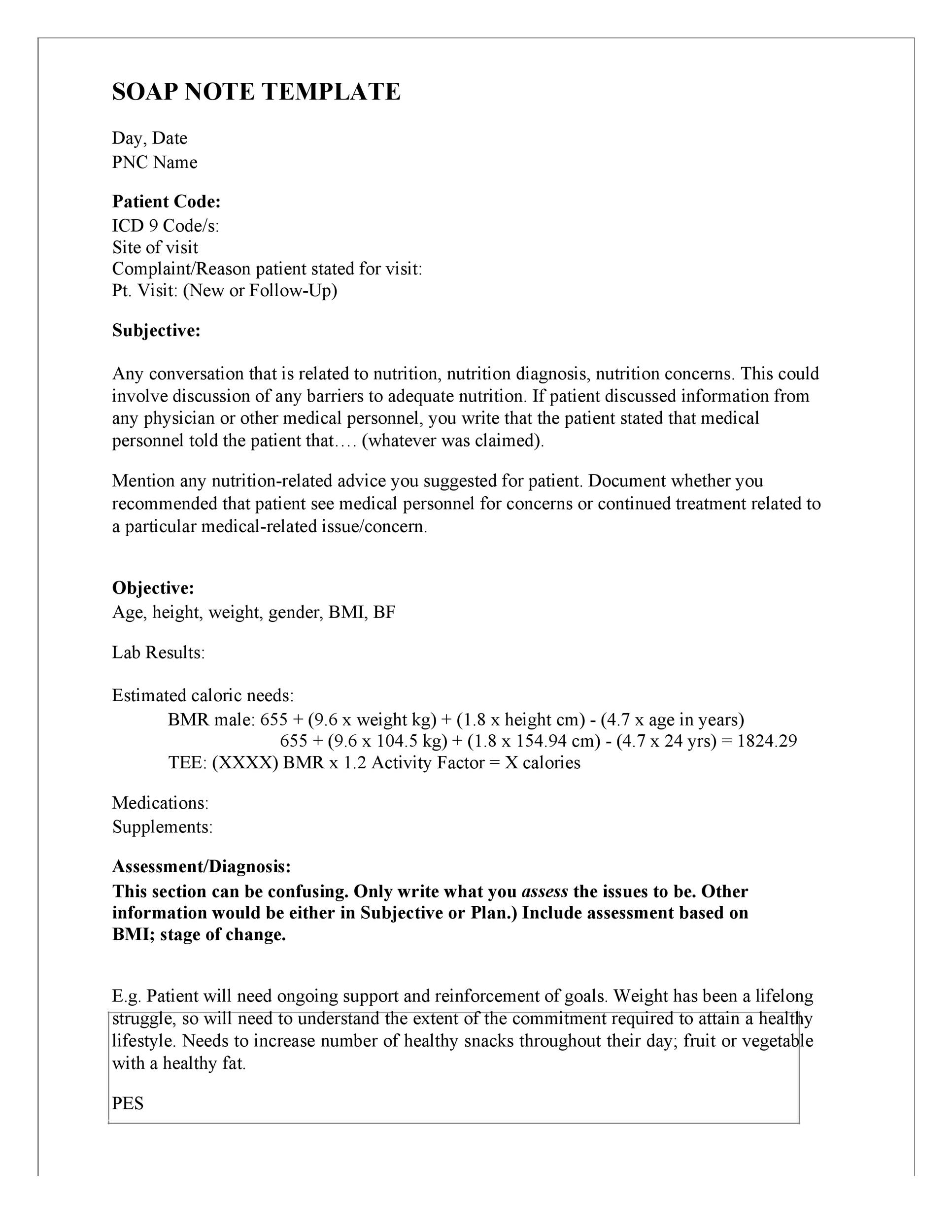
5. Assessment
This section summarizes the clinician’s assessment of the patient’s condition. It’s a concise statement of the diagnosis or differential diagnosis.

- Diagnosis: Clearly state the primary diagnosis (if known).
- Differential Diagnosis: List other possible diagnoses that need to be considered.
- Severity: Assess the severity of the condition.
6. Plan
This section outlines the treatment plan and recommendations for further care.
- Diagnostic Tests: Specify any tests that will be performed (e.g., blood tests, imaging studies).
- Medications: Recommend medications, dosages, and administration instructions.
- Therapies: Outline any therapies (e.g., physical therapy, occupational therapy).
- Follow-up: Schedule follow-up appointments and provide instructions for home care.
Formatting and Best Practices for Pediatric Soap Notes
Consistency and clarity are key when creating and utilizing pediatric soap notes. Here are some best practices:
- Use a Consistent Format: Adhere to a standardized template to ensure all information is captured consistently.
- Use Clear and Concise Language: Avoid jargon and use language that is easily understood by clinicians.
- Be Objective: Focus on factual observations and avoid subjective opinions.
- Use Bullet Points: Break up large blocks of text with bullet points to improve readability.
- Include Visual Aids: Consider adding diagrams or illustrations to clarify complex information.
- Digital Format: Many pediatric practices now utilize electronic soap notes. Ensure the template is compatible with digital platforms.
- Review and Update: Regularly review and update the soap note template to ensure it remains relevant and accurate.
The Role of Technology in Pediatric Soap Note Creation
The rise of electronic health records (EHRs) has significantly impacted the creation and management of pediatric soap notes. While paper-based notes still have their place, EHRs offer numerous advantages, including:

- Streamlined Workflow: EHRs automate many aspects of the note-taking process.
- Improved Data Security: EHRs provide enhanced security and privacy.
- Enhanced Interoperability: EHRs can easily share information with other healthcare providers.
- Real-Time Access: Clinicians can access patient information quickly and easily.
Conclusion
A well-structured and consistently utilized pediatric soap note is an indispensable tool for healthcare professionals. By understanding the core sections, adhering to best practices, and leveraging technology, you can ensure that these vital documents are accurate, complete, and readily available to support optimal patient care. The Pediatric Soap Note Template is more than just a document; it’s a critical component of patient safety and efficient healthcare delivery. Investing in the proper training and implementation of a standardized template will undoubtedly yield significant benefits for both clinicians and patients. Remember, the goal is to provide clear, concise, and actionable information that empowers healthcare providers to deliver the best possible care.